
Peptides
Definitions
Peptide Synthesis
Pharmacy types
Labs
Peptides
SARMS
Definitions
Biologic
Biological products are defined as “a virus, therapeutic serum, toxin,
antitoxin, vaccine, blood, blood component or derivative, allergenic
product, protein, or analogous product, or arsphenamine or derivative of
arsphenamine (or any other trivalent organic arsenic compound),
applicable to the prevention, treatment, or cure of a disease or condition
of human beings”.
• Biological product definition revised in BPCIA of 2009 to include
“protein”
• 2020 – added that chemically synthesized material is included in
definition
• FDA defined a Protein as any alpha amino acid polymer with a
defined sequence greater than a total number of 40 amino acids
(even if comprised of several shorter polypeptide chains).
• March 23, 2020 – FDA Biologic definition updated
– > 40 amino acids: Protein – Must have Biologics License Applications (BLA)
– ≤ 40 amino acids: Peptide
– Synthetic material inclusion in biologic definition
• Removal of human chorionic gonadotropin,
hyaluronidase, follicle stimulating hormone (FSH or
urofollitropin), tesamorelin acetate, and menotropins
“Metaflammation”
• Also know as “Inflammaging” and metabolism induced inflammation
• Chronic low‐grade inflammatory sequela induced by alterations in metabolic signaling
• Increases aging processes and metabolic signaling issues
• Endoplasmic reticulum stress reported key to excessive inflammatory response
Caused by AND leads to “diabesity”:
– Insulin resistance; type 2 diabetes
– Obesity
– Stress
– Diet
– LPS induced GUT issues and inflammation
– Liver / kidney issues
Stress causes cravings, sleepdisturbance and weight gain
• Cortisol – DHEA ratio
• Insulin resistance follows
• Weight gain leads to adiponectin
alterations and loss of AMPK in
the cell
. . . the inflammatory cycle begins
Peptides
• Short chains of amino acids linked By amide bonds
• < 50 amino acids
• Less likely to evoke immune response when administration
• Peptide from Greek word meaning “to digest”
• Played a role in therapeutics since the 1920s – insulin
• High specificity and affinity for target
• Highly efficacious, good tissue penetration
• Low allergenicity
• Natural compounds
• Safe, well tolerated
• Fast clearance
• Low Toxicity
• Over 7,000 naturally occurring peptides identified
• Crucial roles in human physiology – improves
metabolic signaling
• Over 100 peptide‐based drugs approved by US FDA in past 30 years
• Market = 14.4 billion in 2011 to almost 28 billion in 2018
• US market 40% of global peptide sales
Examples of FDA Approved Peptides Already on the Market:
• Erythropoietin – RBC production
• Sermorelin acetate – diagnostic for pituitary function;
increases growth in children
• Tissue plasminogen activator (TPA)‐ heart attack/stroke
• Oxytocin – maintain labor pain ; “cuddle” hormone ‐
improve sexual libido; also may help with decreasing opiate
withdrawal
• Bradykinin – improve peripheral circulation
• Somatostatin – decrease bleeding ulcer
• Gonadotropin – induce ovulation
• Insulin – maintain blood glucose level
• Bremelanotide (Vyleesi) – Female or Male Sexual
Dysfunction
• Zadaxin – Thymosin Alpha1 for Hepatitis B and C
• Semaglutide GLP‐1
• Tirzepatide mixed GLP‐1
Potential General Side Effects from Peptide Injections
• Itchy at the injection site
• Redness at the injection site
• Water retention ‐ most likely need to reduce dose
• Increased hunger
• Dry mouth
• Nausea
• Tingling or numbness in the extremities (toes,
fingers – reduce dose)
• Increased hair and nail growth
Current Regulatory Environment
• FDA clamping down on Compounding Pharmacies ability to
manufacture and sell high quality, highly therapeutic and SAFE
peptides
• FDA issued at 503‐A compounded products now have many
peptides added to “category 2”
• FDA considers category 2 peptides to be banned from bulk
drug compounding
• “raise significant safety risks”
• Several law‐suits on this issue are currently in the system
• According to FDA, the term “protein” is distinct from and excludes
the term “peptide” (i.e., amino acid chains that are generally
shorter and simpler than a protein).
• FDA uses “bright-line rule” based on number of amino acids in an
amino acid polymer regardless of method of manufacture.
• But FDA uses fact-specific, case-by-case analysis for amino acid
chains not found in naturally occurring proteins.
• Between 2015–2019, the U.S. Food Drug Administration (FDA)
authorized a total of 208 new drugs (150 new chemical entities and
58 biologics), 15 of which were peptides or peptide-containing
molecules.
A (compounded) peptide is regulated as a drug under the
FD&C Act unless the peptide otherwise meets the statutory
definition of a “biological product” (>40 amino acids) and is
therefore regulated under the Public Health Service Act.
History of Commonly Used Peptides
• Before April 2020
• FDA and State Boards of Pharmacy did not specifically indicate that certain
peptide bulk drug substances were an issue and provided little to no objection
to the practice.
• After April 2020
• The tides changed after an FDA warning letter issue sometime in April 2020
identifying multiple peptides used in practice today.
• FDA indicated these products were not in conformance with 503A and not eligible for compounding.
• Indicated that nomination with sufficient data and lack of FDA safety concerns may have cured deficiency.
• State Boards of Pharmacy became emboldened after an October 2020 DOJ guilty
plea by a pharmacy to a single count of manufacturing an unapproved drug.
• Confusion exists on how a single count of unapproved drug manufacturing can encompass numerous bulk
substances primarily compounded separately.
Physician Marketing 101
• Do not make claims!
• The use of may and has been shown
• Provide supporting evidence
• Websites are being monitored!
• Drug pricing
• Don’t put yourself under FDA regulation
USP 2020–2025 Biologics
USP Monographs
• Expert Committee Established!!
• Mission
• The Biologics Monographs 1 – Peptides & Oligonucleotides Expert Committee is responsible for
the development and revision of USP-NF monographs and their associated USP Reference
Standards in peptides and oligonucleotides
• Focus
• Monographs and reference standards (RS) for synthetic, recombinant, naturally-derived
therapeutic peptides under 40 amino acids in length
• Quality control of raw materials used in manufacturing of synthetic peptides
• Selected general chapters that pertain to peptides and oligonucleotides
• Modernization of outdated monographs
• Identification and development of new monographs and RS
• Key Issues
• Work with other Biologics Expert Committees, FDA and stakeholders to improve existing peptide
monographs and develop new peptide monographs
• Conduct workshops relevant to areas of interest to the Expert Committee
• Transition from recombinant to synthetic drug and regulatory considerations and reference
standards needed to support both forms
Beyond Compounding…
• Online Peptide Sales
– Legal Statements:
• “By placing orders with this company it we understood by the buyer that under no
circumstances should use any of these chemicals/materials in an inappropriate manner.
No products here are to be used for recreational purposes or human consumption. All
customers are assumed and expected to be qualified researchers.”
• “Products on this website are sold for laboratory research purposes only. The
information provided on this website and the products offered on this website are for invitro
lab research use only. The products are not medicines or drugs and they have not
been approved by the fda to prevent, treat, diagnose, mitigate, or cure any disease,
ailment or medical condition. ALL ARTICLES AND PRODUCT INFORMATION PROVIDED
ON THIS WEBSITE ARE FOR INFORMATIONAL AND EDUCATIONAL PURPOSES ONLY. The
products offered on this website are not for human or animal consumption of any
kind.”
– Quality:
• The purchaser agrees that the products have not been sterilized or tested for safety and efficacy in food, drug, medical device, cosmetic, commercial or any other use.
Unique Class of Pharmaceutical Compounds
Molecularly poised between small molecules &
proteins
As signaling molecules, therapeutic intervention
closely resembling natural pathways
Natural sources Synthetic Exotic sources
Ligands Analogs Conjugation
Native – Analogs – Heterologous
60+ Peptides approved in U.S., E.U., Japan
150+ in active clinical development/trials
~260 tested in human clinical trials
500+ in preclinical development
More than 3,200 antimicrobial peptides (AMPs) have
been discovered, nine of which have been
approved by the U.S. Food and Drug Administration
(FDA).
PEPTIDE CONJUGATES
Represent an important class of
therapeutic agents that combine
one or more drug molecules with a
short peptide through a
biodegradable “linker”.
This prodrug strategy uniquely and
specifically exploits the:
(a) biological activities and
(b) self-assembling potential of
small-molecule peptides
to improve the treatment efficacy
of medicinal compounds.
RESEARCH USE = UNREGULATED
RUOs are defined very briefly by FDA regulations:
Commercial RUO products are described as products “in the laboratory research phase of
development and not represented as an effective in vitro diagnostic (therapeutic) product.”
RUO products must bear the following labeling statement:
“For Research Use Only—Not for Use in Diagnostic Procedures.” (Although not authorized by
the regulation, many companies have shortened the statement to just the first-half of the clause).
FDA regulations do not define any other restrictions/limitations on RUO products beyond this
labeling statement.
FDA regulations define the category and labeling . . . and nothing more.
Not clear that they are even subject to FDA’s jurisdiction.
Aside from bearing the mandated statement, the manufacturing of RUO products:
Do NOT need to be listed with FDA or comply with ANY Quality System Regulation (QSR).
Can be sold (for research) without any FDA clearance or approval.
Unregulated by FDA.
RESEARCH USE ≠ CGMP
Products labeled RUO are not required to be manufactured in accordance with cGMP and FDA Quality System Regulation. “. . . the lack of manufacturing controls may be detrimental to the quality of the control material. As such, clinical laboratories using RUO quality control materials to ensure the quality of testing may be placing patients at unnecessary risk.”
https://microbiologics.com/
Are RUO and IUO products required to be manufactured in compliance with the Quality
System regulation?
FDA does not require RUO products or IUO products . . . to be manufactured in
compliance with the Quality System (QS) regulation (21 CFR 820).
In addition to overt expressions by the manufacturer (such as those present in labeling and advertising), intended use may be “shown by the circumstances surrounding the distribution of the product and the manufacturer's knowledge that its product is offered and used for a purpose for which it is neither labeled nor advertised.”
RESEARCH USE ≠ FDA APPROVAL
RUO products are essentially unregulated in the U.S. but must be branded with
the statement: “For Research Use Only. Not for use in diagnostic procedures”.
Labeling a product as such permits it to be used by researchers, who can
evaluate usefulness for a specific diagnostic purpose.
“RUO manufacturers do not have to register or list their RUO products with FDA or
comply with manufacturing standards.”
https://regulatoryandmore.com/
RUO products can be legally offered for sale without any FDA knowledge,
clearance, oversight, or approval.
FDA & RUO/IUO PRODUCTS
DOCKET NUMBER: 2011-D-0305 (LINK TO FDA FINAL GUIDANCE DOCUMENT)
“FDA is concerned that distribution . . . has led to . . . the use of products
with manufacturing controls that are inadequate . . .”
Intended Use:
Refers to the “objective intent” of those responsible for labeling the product.
Intent may be shown by the circumstances surrounding the distribution of product.
Merely placing RUO/IUO on the label does not render it exempt
Determined by other evidence, including how the product is marketed
Product design; statements; claims; clinical info; workshops; presentations
Misbranded; 502(a) & 502(o) of 21 U.S.C. 352(a), 352(o)
Adulterated; 501(f) of 21 U.S.C. 351(f)
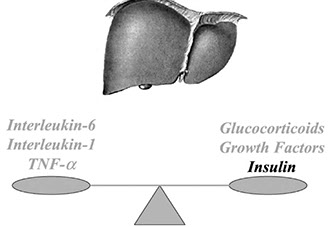
Metaflammation Induces Catabolic State

Balance of Pro‐ and Anti‐inflammatory compounds
regulate acute phase response of inflammation


Peptide Synthesis
SIDE-CHAIN PROTECTING
GROUPS FOR FMOC AMINO
ACIDS
“Linkers” provide point of attachment for
the C-terminal amino acid.
Most cleavage/deprotection methods are
TFA-based, and they differ primarily in:
the final concentration of TFA
types of scavengers used
reaction times
Mainly dictated by the amino acid composition of the peptide.
BUILDING A PEPTIDE
• Made of amino acids linked together in a chain-like structure
• Fluorenyl methoxycarbonyl (Fmoc) protecting group
• Prevention of unwanted reactions
• Must be removed from NH2 side, but left on the COOH
• R-group requires protection as well
• SPPS developed by chemist Bruce Merrifield in 1963
• AA preloaded to resin; successive Fmoc removal/coupling
Cleave peptide from resin;
Trifluoroacetic acid (TFA)
• Must perform salt exchange with Acetic or HCl Acid
TFA CLEAVAGE COCKTAIL
FORMULATIONS – HIGH % TFA
Structure of the linker:
determines method of cleavage
peptide functionality
Low %TFA: XAL (“Seiber”) or HAL
High %TFA: PAC (“Wang”), PAL, AM, or BAL
Source: Thermofisher
TFA: trifluoroacetic acid
TIPS: triisopropylsilane
EDT: 1,2-ethanedithiol
DTT: dithiothreitol
TES: triethylsilane
DCM: dichloromethane
TRIFLUOROACETIC ACID/ACETATE EXCHANGE
Prepare a small column of strong anion exchange resin
Elute the column with a 1M solution of Sodium Acetate
Wash column with distilled water removing excess
Sodium Acetate
Dissolve peptide in distilled water and apply to column
Elute the column with distilled water and collect fractions
containing the peptide
Lyophilize peptide containing fractions to obtain the
peptide acetate salt
• (reconstitute/repeat lyophilization step 2-3x)
TRIFLUOROACETIC ACID (TFA)
The dose level of 160mcg/mL of sodium trifluoroacetate is considered
to be the NOAEL in both sexes; approximately equal to:
8mg - 10mg TFA/kg body weight/day in males and females, respectively.
organ weights and organ+body weight ratios; Hgb, Hct, Bilirubin, Glucose,
ALT/AST
https://echa.europa.eu/registration-dossier/-/registered-dossier/5203/7/6/2
Cornish J, et al. Am J Physiol. 1999 Nov;277(5):E779-83. doi: 10.1152/ajpendo.1999.277.5.E779.
inhibits proliferation of osteoblasts and chondrocytes
Cousins M, et al. Anaesth. Intens. Care (1979), 7, 9
Hepatotoxic, Neurotoxic
Binds to hepatic proteins forming neoantigens, responsible for
production of autoantibodies against liver tissue
SOURCING PEPTIDES
Chemicals Must Minimally Be:
• From FDA registered Manufacturer
• https://www.accessdata.fda.gov/scripts/cder/
drls/default.cfm
• Accompanied by a valid C of A
Contain Identifiers:
• MF, CAS, A.A. Sequence, MW
Include Tests:
• Appearance
• H2O (and CH3COOH) content
• Assay/Purity
• Impurities
Lot, Storage, Expiration, etc
CALCULATIONS FOR PEPTIDE PRODUCTS
Summary of Calculations
I. Determine correct chemical & observe assay or potency.
II. Remove and/or account for impurities, assay, and water content
(actual peptide content) . . .
III. Solve for the API that is left in the remaining chemical based on the
assay/purity.
IV. Decide if there is need make further corrections for the salt-form in
the chemical.
V. Any other considerations that may apply to the chemical being
used.
CALCULATIONS FOR PEPTIDE PRODUCTS
Summary of Calculations
I. Purity . . . . . . 99.5%
II. H2O . . . . . . . . 5.1%
III. CH3COOH . . . 10.8%
• (0.995) x (0.949) x (0.892) = 84.2%
If making 5L @ 2mg/mL: requires 10gm … however, 11.9gm needed
to obtain required concentration.
STERILE FILTERING OF SOLUTIONS - 21 CFR 211.113 (B)
1. Appropriate to Use
• Material/Size
2. Sterilization of the Filter
• Irradiation, Autoclave
3. Stability of the Filter Used
• Filter construct material
interaction with product/pH
4. Binding on the Filter
• Contact surfaces do not bind
any formulation component
5. Compatibility of the Filter
• Chemical/Bio-compatibility
6. Extractables/Leachable
• Distressed/Normal conditions
7. Bacterial Retention
• B. diminuta (ATCC 19146)
• 1 x 107
• ASTM F838-05
8. Integrity Testing
• Bubble point
• Forward flow/Pressure hold
Stability of Peptides
• The shelf-life of peptides in solution is very limited.
• Especially true for peptides whose sequences contain:
• Cys, Met, Trp (oxidation) . . . or
• Asp, Gln, Arg, Lys, His, and N-terminal Glu
• Minimize exposure to air
• Avoid freeze-thaw cycling (degradation, pH shifts, etc.)
• Keep Refrigerated (what if . . . )
QUALITY CONTROL IN THE PHARMACEUTICAL
COMPOUNDING OF STERILE PRODUCTS
503A – USP <795> and <797>
Compounding by a licensed pharmacist/pharmacy or physician
“For an identified patient based on unsolicited receipt of a valid prescription . . . Or
notation that compound is necessary for patient”
Copies of marketed products should not be in “inordinate amounts” (i.e. > 4 units/month)
Chemicals must comply with USP monographs, if exists
If monograph does not exist, must be components of approved drugs
If neither available, bulk drug substance must:
• Be from FDA registered MFG under 510 of FD&C Act [207.3(a)(4) of Title 21 CFR]
• Be accompanied by a valid C of A
CFR21: § 216.23 Bulk drug substances that can be used to compound drug
products in accordance with section 503A of the Federal Food, Drug, and
Cosmetic Act:
(1) Brilliant Blue G
(2) Cantharidin (topical use only).
(3) Diphenylcyclopropenone (topical use only).
(4) N-acetyl-D-glucosamine (topical use only).
(5) Squaric acid dibutyl ester (topical use only).
(6) Thymol iodide (topical use only).
Personnel Garbing and Gloving
Prior to and during aseptic compounding
Particles generated ≥ 0.3μ/minute; slow walk (smock: 5,000,000 vs coverall: 500)
> 10 million particles >0.3μ per 1 ft2 of the cleanest hands
Personnel training and evaluation in aseptic manipulations and sterilization skills semi-annually***
PPE Gowning, Didactic Training, Written Competence, Skill Assessment, Cleaning, Media Fills
Environmental quality specifications & monitoring
Air and surface sampling (required every 6 months***; but often performed more frequently)
Temperature: ≤ 20°C (68°F) or cooler
Humidity: 35% to 60%
Routine and Scheduled Disinfection of gloves/surfaces within ISO-5 sources NLT every 30 minutes
503A – FACILITY DESIGN
1° Engineering Controls (LAFW, BSC, CAI, CACI, etc.) – (ISO-5)
Unidirectional @ ~90fpm; smoke studies
2° Engineering Controls – (Buffer area, Ante; Prep) – (ISO-7/8)
Differential Pressure
> 0.02 (to 0.05) inch water column between adjacent areas (5-12 Pascals)
NLT 30 ACPH: [CFM x 60 / (Area x Height)]
503A – ADOPTION OF USP <797>
03/2021: 39 State Boards of Pharmacy require full
compliance
An additional 11 states have strong requirements on
sterile compounding practice—which 10 states
characterize as “equivalent to or stricter than”
Chapter <797>
2015: Only 26 states required <797> or equivalent
quality standards for sterile compounding.
39 states prohibit traditional pharmacies from
compounding sterile office stock for humans.
11 states have office stock policies (many predating
the federal law) that are not aligned with federal
statute
503B –
Can compound large batches of medication to be dispensed to clinics, doctors’ offices
and other healthcare facilities for general office use.
Must comply with cGMP & submit documentation of processes and testing results.
May not compound a drug product from bulk drug substance unless:
1. the bulk drug substance appears on a list identifying bulk drug substances for which there
is a clinical need (the 503B bulks list), or
2. the drug product compounded from bulk drug substance appears on FDA’s drug
shortage list at the time of compounding, distribution, and dispensing.
Chemicals must comply with USP monographs if exists
If monograph does not exist, must be components of approved drugs
If neither is available, bulk drug substance must:
• Be from FDA registered MFG under 510 of FD&C Act
• Be accompanied by a valid C of A
Added 4/6/23 – Federal Register
Quinacrine HCl (for oral use only)
NOT Included on list for 503B
Hydroxyzine HCl Mannitol
Methacholine Chloride Metoclopramide HCl
Nalbuphine HCl Potassium Acetate
Procainamide HCl Sodium Bicarbonate
Sodium Nitroprusside Verapamil HCl
503B – USP <795>, <797>, 21 CFR Part 210 and 211 (cGMP)
Part 210: Minimum practices in manufacturing, processing, packing, or
holding of all compounded drugs
Part 211: Refers specifically to the requirements of finished pharmaceuticals
Requirements of <797> found in 503A, PLUS:
Increased Environmental/Personnel Monitoring Frequency
Required product validation testing
components/container closure/method suitability/sterility/stability
maximum batch size & time parameters
Documentation requirements
503B – cGMP
1. Facilities/Equipment
a) HEPA-filtered air @ ISO-5 quality
i. Leak tests and velocity uniformity biannually
ii. Smoke Studies; Under dynamic conditions
b) Supporting Clean Areas = ISO-6,7,8
c) ACPH (e.g., ISO-8 = 20 ACPH)
d) Pressure Differentials: 10-15 Pascals (0.04-0.06 inches water column)
e) Construction Materials (e.g., FRP walls; sealed ceiling tiles, easily cleanable)
f) Airlocks & Passthroughs
503B – cGMP
2. Personnel
• Technique, behavior, microbiology, hygiene, gowning, SOPs, etc.
3. Components/Containers/Closures
• API, SWI, Excipients (bioburden)
• Use of SWI for final rinse prior to sterilization/depyrogenation via dry heat
4. Endotoxin
• Not removed via sterile filtration - - chemicals must but be of pure quality
503B – cGMP
5. Time limitations to be established for each phase of production in compounding process
6. Validations of Aseptic Processing/Sterilization
• Media fills/Frequency, Duration, Size of batches
7. Laboratory Controls
• Active & Passive Air Monitoring (settling plates)
8. Sterility Testing
• USP<71>, Investigations, RCA
9. Documentation
503B - VENDOR EVALUATION
1. Ensure licensure is in place
2. Familiarize yourself with their regulatory history
• (FDA inspections with OAI (Official Action Indicated)
3. Review the number of SKUs they report in a 6-month period (503B only)
4. Examine any recall information and purpose thereof
5. Verify the annual drug review for the FDA (cGMP requirement for 503B)
6. Check references from customers with similar operations …
• *(beware of bad review trolls on internet)* - - (Reservations analogy)
7. On-site visit - - know what to look for ahead of time - - review <797> (or cGMP for 503B)
• evaluation based on the quality system in place and compliance with quality guidelines
8. ** know how to interpret the findings of a 483 ** request responses to 483 observations
(transparency)


QUALITY CONTROL IN THE PHARMACEUTICAL
COMPOUNDING OF STERILE PRODUCTS

Pathophysiology
HYPOTHALAMUS
Connects the nervous system to the endocrine system
GONADOTROPIN- RELEASING HORMONE
(GnRH)
CORTICOTROPIN RELEASING HORMONE (CRH)
THYROTROPIN RELEASING HORMONE (PROLACTIN RELEASING HORMONE) (TRH)
GROWTH HORMONE RELEASING HORMONE (GHRH)
SOMATOSTATIN (GH INHIBITING HORMONE)
PROLACTIN INHIBITING HORMONE
HPA IS ACTIVATED BY PEPTIDES
The main activator of the HPA axis is the neuropeptide corticotropin-releasing hormone
(CRH) synthetized in the hypothalamic paraventricular nucleus (PVN)
CRH is released into the portal vessels of the median eminence to the pituitary
CRH release leads to synthesis and release of adenocorticotropic hormone (ACTH)
HYPOTHALAMUS TO ANTERIOR PITUITARY
Hypothalamic hormones travel through hypothalamo-pituitary portal circulation to anterior
pituitary and bind to receptors on surface of pituitary.
As a consequence the pituitary will start or stop secreting hormones into the systemic
circulation.
ANTERIOR PITUITARY
TSH
ACTH
GH
FSH
PROLACTIN
LH
POSTERIOR PITUITARY
Sometimes considered extension of hypothalamus
OXYTOCIN
VASOPRESSIN
ADRENAL GLANDS
ADRENAL CORTEX
Steroid
• mineralocorticoids (aldosterone)
• glucocorticoids ( cortisol and corticosterone)
• androgens
ADRENAL MEDULLA
Catecholamines
• epinephrine
• norepinephrine
CLASSIFICATION OF HORMONES
PEPTIDE/PROTEIN
(<50 aa) and polypeptide (protein) > 50 aa- insulin, ADH, FSH, ACTH, prolactin,
ghrelin, glucagon, GH, FSH, renin, TSH, glucagon-like peptide (GLP-1), oxytocin,
calcitonin, parathormone, thymulin, anti-Mullerian hormone, T3,Gastric inhibitory peptide,
somatostatin, Insulin-like growth factor, brain natriuretic peptide, endothelin,
thrombopoietin, adiponectin, lepsin, galanin, cortistatin, vasoactive intestinal peptide
STEROID made from cholesterol- estrogen, progesterone, testosterone,
androstenedione, dehydroepiandrosterone (DHEA)
TYROSINE (AMINE)- thyroxine, dopamine and catecholamines (epinephrine and
norepinephrine)
EICOSANOID- thromboxanes, leukotriens, prostaglandins, prostacyclin
PEPTIDE/POLYPEPTIDE PROTEIN/HORMONES
Made up of amino acids +/- other molecules (eg. CHO )
Large or small hydrophilic molecules
Synthetized in the rough ER transferred to Golgi, repackaged into vesicles to be excreted
Stored until the signals are received for secretion
Freely transported through blood stream
Receptors inside nucleus
Bind to DNA to modify transcription
Rapid/temporary action
STEROID HORMONES
Secretions of ductless glands
Made from cholesterol
Small hydrophobic molecules
Synthesized in the smooth ER
Synthesized as needed
Attach to protein carrier for transport in blood stream (eg. SHBG- testosterone)
Receptors on cell surface- their signaling affects change in the cell
Serve as second messengers
Slow/permanent action
Eg. Estrogen, Testosterone, Cortisol, Aldosterone, Progesterone
TYROSINE DERIVATIVE HORMONES
Derived from L- tyrosine
One amino acid is manipulated to make hormones
Act either way steroid or protein
Thyroid T4- steroid like
Catecholamines- Epinephrine and Nor-epinephrine- protein and polypeptide
PEPTIDE INFLUENCE ON HORMONE FUNCTION
Protection of cellular efficiency (improves metabolism, reduce oxidative stress)
Monitor and influence timing of cellular senescence (longevity)
Modulate inflammatory response (decrease oxidative stress)
Repair & Restore (cellular repair)
Adjuncts to hormone therapy and improve hormone balance and metabolic function at
cellular and nuclear levels
Every cell in our body has hormone receptors and peptides message these receptors
Clinical Effects of Excessive HPA axis Activation

Glycolysis
In the cytoplasm
Does not require oxygen
“Investment phase” uses 2 ATP
C6H12O6
C-C-C-C-C-C (glucose) +2 ATP ->2 P-C-C-C + 2 ADP
“Payoff phase” uses 2 NAD+ and Mg++ -> 2 pyruvate +4
ATP and 2 NADH for electron transport chain
Net gain 2 ATP
Acetyl CoA
Can come from glycolysis producing 2 pyruvate
Each pyruvate (3C) to Acetyl CoA(2C) reduces NAD+ to
NADH and yields Co2
Can come from protein or fat
Net 2 NADH for electron transport chain
Ketones bypass need for this
Kreb/Citric Acid/TCA cycle
Occurs in matrix of mitochondria
Acetyl CoA(2C) merges with oxaloacetic acid(4C) to form citric
acid (6C)
Reduces 3 NAD+, FAD+, one ADP (heart) or GDP (liver)
Each pyruvate produces two CO2, 3 NADH, and 1 FADH2, ATP
for the electron transport chain
Process occurs twice because one glucose(6C) produces two
pyruvate (3C)
Inhibited by ATP and NADH
Oxidative phosphorylation
In the mitochondrial matrix, too
NADH oxidized to NAD+, losing electrons “reduced”
Intermediary acceptors are CoQ and cytochromes I-IV in
phospholipid bilayer of inner mitochondrial membrane
Release of energy pumps hydrogen ions into intermembrane
space, creating a gradient
This gradient is used in transmembrane protein ATP Synthase
to create ATP
Eventual acceptor of these electrons is oxygen (O2), which
splits to form water (H2O)
Energy Yield
30-38 ATP
In a real cell, some ATP is used to transport ADP into the Matrix
Some ATP is used to transport ATP out of the mitochondrion
Some ATP is used to transport other molecules
2 net ATP in glycolysis
2 net ATP in citric acid cycle
All depends on the metabolic state of the cell
Glycogen
Polysaccharide of glucose
An energy reserve that can be quickly mobilized
Stored in cells without disrupting osmotic pressure (vs glucose)
Stored in liver and muscle, small amount in glial cells of brain
Fasting causes release of glycogen for use in Glycolysis
Glycogen in muscle is solely available for muscle use b/c muscle lacks G6P to move
glucose out of the cell
Glycogen breakdown impedes muscle uptake of glucose from blood, increasing
blood glucose for other tissues like brain
Fermentation/Glycolysis
Glycolysis in the absence of oxygen as an electron acceptor
In yeast, makes alcohol
In muscle tissue, makes lactic acid
In RBC’s without mitochondria, only lactic acid fermentation occurs
Pyruvate takes 2 NADH from glycolysis and produces 2 lactate plus 2 NAD+
Lactic acid from muscle cells transported via blood to liver where it’s converted
back to pyruvate for normal cellular respiration
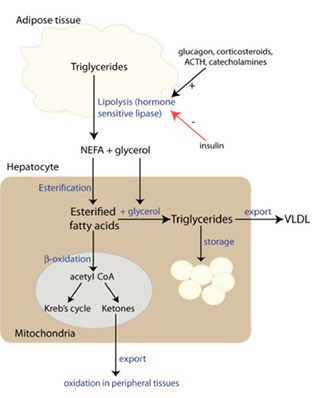
Beta oxidation
Also occurs in mitochondrial matrix
Triacylglycerol (TAG) in adipocytes and striated muscle
Stimulated by epinephrine, ACTH
CD36 transport protein
Adipose tissue hormone sensitive lipase (HSL).
Fatty acid tails broken into 2 carbon units that combine with CoA
forming acetyl CoA for the Kreb cycle
Beta oxidation releases FADH2 and NADH for ETC inside IMM
Intracellular fatty acid intermediates can be toxic
All depends on the metabolic state of the cell
Osteoarthritis
◦ Chondrocytes in OA joints develop terminal differentiation and hypertrophy
(like adipocytes) near sites of trauma
◦ Secrete type X collagen (matrix mineralization),
◦ Secrete transglutaminases (creating modified immunogenic peptides),
and
◦ Release vesicles containing calcium phosphate crystals
◦ 120 70-ish, mostly male patients with end stage OA undergoing TKA
◦ 100% showed articular cartilage mineralization primarily BCP
◦ Degree of mineralization correlated with histologic cartilage destruction
◦ Basic calcium phosphate (BCP) crystals
◦ activate synovial macrophages to drive inflammation
◦ Leads to an imbalance in anabolic/catabolic mediators
◦ Upregulation of metalomatrix proteinases, NFKb, TNFa, IL6, IL1b,
inflammasome
◦ Fuerst, M. Calcification of articular cartilage in human osteoarthritis. Arthritis & Rheumatology. 2009;60(9):2694-703.
◦ Aeschlimann, D. P2X7 receptor-mediated TG2 externalization: a link to inflammatory arthritis? Amino Acids. 2017;49:453-60.
◦ Cunningham, C. Osteoarthritis-associated basic calcium phosphate crystals induce proinflammatory cytokines and damage-associated molecules via activation of Syk and PI3 kinase. Clinical Immunology.
2012;144(3):228-36.
◦ Millerand, M. Danger signals nd inflammaging in osteoarthritis. Clin and Exp Rheumatol. 2019;37(s120):s48-s56.
Macrophage
Innate immune cell
Activates in response to injury/illness
Pathogens- fungal, bacterial, protozoal, viral
Toxins- environmental, food, protein byproducts of disease
Chronic stress, sleep disruption
Trauma
Autoimmune conditions
Abundance of misfolded proteins
Generates ROS for coping with these
Macrophage activation with canonical microbial compounds
such as lipopolysaccharide (LPS), a specific Toll-like receptor 4
(TLR4) ligand, leading to classically activated (M1)
proinflammatory macrophage generation. This activation
induces an increased glycolysis and a disrupted Krebs cycle, in
order to supply cell metabolic adaptations and cytokine
production. On the other hand, macrophage stimulation with
interleukin 4 (IL-4) generates alternatively activated (M2) antiinflammatory
macrophages. In this case, cells rely on fatty acid
oxidation (FAO) and oxidative phosphorylation to support the
metabolic program initiated by IL-4.
The Cell has a Choice
The Efficient cell has Metabolic Flexibility:
lots of NAD+ and ATP
not too many ROS, plenty of antioxidants
Excess glucose/lipid, dysbiosis are stressors
The intelligent cell has a choice: autophagy, apoptosis, senescence
The cell takes on a hyperglycemic phenotype:
Upregulates citrate, glycolysis, cholesterol synthesis
Downregulates fatty acid oxidation, BCAA metabolism, ox phos in general
Creates an increased state of ROS- another stressor
Burns through ATP and NAD+
Increases NADPH to deal with increased ROS
Hyperglycemic phenotype
Slows down, upregulates mTOR, upregulates fatty acid synthetase
ER stress with misfolded proteins
Nucleus turns on p53 to stop the cell cycle and handle the stress
Can pull in the immune system for autophagy/mitophagy, apoptosis or
senescence
BUT the T cells are also affected by hyperglycemia
Inefficient
Competing for increasingly limited NAD+ and ATP
Spewing inflammatory cytokines
ER Stress and the UPR
In resting “conditions’’, ER receptors are kept inactive by binding to the ER molecular chaperone GRP78
In ER stress, normal protein processing is hindered, which results in an accumulation of unfolded or misfolded
proteins in the ER lumen.
This accumulation triggers a cascade of signal transduction called unfolded protein response (UPR). UPR is
controlled by three transmembrane sensors : PKR-like ER kinase (PERK), inositol-requiring enzyme 1α (IRE1α),
and activating transcription factor 6 (ATF6).
When the ER homeostasis is disrupted, GRP78 detaches from these three receptors, initiating further downstream
signaling cascades leading to decreasing protein synthesis in attempt to reduce the burden of misfolded proteins,
enhancing synthesis of molecular chaperones, and activating a proteasomal degradation process called the ERassociated
degradation (ERAD) pathway.
The UPR is primarily adaptive, however, when the stress is severe, UPR may activate apoptosis.
In humans, defective protein folding is believed to be one of the key molecular hallmarks of disorders such as
diabetes, obesity, neurodegeneration, or cancer.
The Inflammasome
In peripheral monocytes, smooth muscle cells, endothelial cells
Stimulation of TLR4 by PAMPS and DAMPS from ischemia, radiation, infection
NFKB transloction to the nucleus
Posttranslational modification of NLRP3: ubiquination, nitrosylation and
phosphorylation
Plus K+ efflux, lysosomal dysfunction leads to Pyroptosis and propagation of
inflammation
Higher levels of NLRP3, IL-1B, Il-18 in patients with AMI/UA
Continued decline in cellular efficiency
Brain and intestinal cells unable to make
neurotransmitters because all need NAD+
limits hypoglycemic effect of serotonin on
the pancreas
Histone acetylation by oxidative stress,
regulating gene transcription
mRNA expression of all SIRT genes reduced
apoptosis no longer an option
Senesence takes over
Senesent cells affect tissue-specific stem cells (repair)
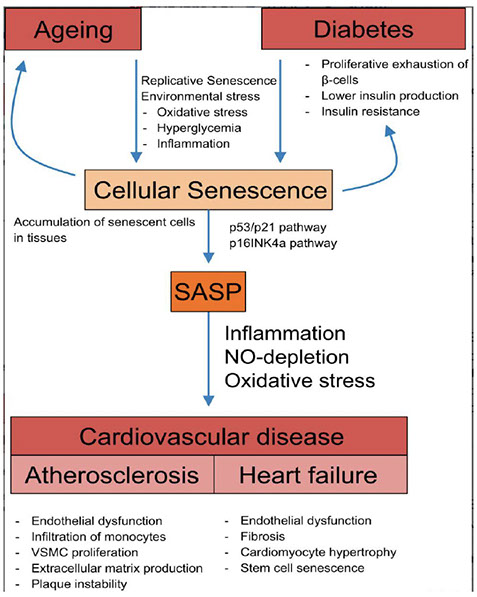
Senescence
Permanent cell cycle arrest
Large cell size
Excessive lysosomal activity producing beta
galactosidase
Senescence associated secretory phenotype
(SASP) of inflammatory cytokines Il6, IL1B, TNFa
Paracrine effects on tissue-specific (PBC,
cardiac endothelial…) stem cells
Tissue non-specific alkaline phosphatase (TNAP) causes degradation of extracellular ATP and ADP to AMP and adenine causes cessation of inflammatory signaling, and induction through adenine receptors of an anti-inflammation response. TNAP has been implicated in protection against inflammation in multiple diseases and promotion of intestinal microbial populations through hydrolysis of extracellular ATP/ADP to AMP and adenosine.
◦ Intestinal AP has been shown to dephosphorylate (detoxify) the lipid A moiety of lipopolysaccharide (LPS), the outer lipid layer of the outer membrane of Gram-negative bacteria. In vertebrates, these phosphates are important for binding of LPS to the toll-like
receptor 4/MD-2 innate immune receptor complex, initiation of NF-kB signaling, and immune
response induction.
◦ Intestinal AP deficiency has been associated with inflammation in the human intestine.
Supplementation of IAP to animals where intestinal inflammation is induced directly or
indirectly (with antibiotic use for example) reduces inflammation. Use of AP as
treatment showed short-term improvement of severity of UC in patients with moderate-tosevere
UC.
◦ Rader, B. Alkaline Phosphatase, an Unconventional Immune Protein. Frontiers in Immunology. 2017;8:897.
◦ Inflammatory bowel disease (IBD), comprising Crohn's disease (CD) and ulcerative
colitis (UC), is characterized by chronic and relapsing inflammation in the
gastrointestinal tract, and some hypotheses propose that damage to the intestinal
mucosa occurs as a result of dysregulated innate immune response.
◦ The innate immune system is the first line defense, which can sense microbes or
endogenous danger signals via recognition of damage-associated molecular
patterns (DAMPs) or pathogen-associated molecular patterns (PAMPs) by host
pattern recognition receptors (PRRs), such as Toll-like receptors (TLRs) and NLRs.
◦ Under normal conditions, a basal level of reactive oxygen
species (ROS) has bactericidal effects, participating in the
intestinal defensive function. However, in the process of chronic
inflammation (such as IBD or PUD), excessive ROS produced by
the infiltrated neutrophil can trigger oxidative stress (OS) and
proteolytic enzymes, which act on endothelial cells and cause
cell injury and subsequent intestinal mucosal barrier damage
and luminal pathogen invasion, and further in turn exaggerate
inflammatory cell infiltration and inflammatory damage,
eventually leading to intestinal mucosal necrosis and ulceration.
◦ ROS could also act as secondary chemical messengers for the
activation of intracellular signal pathways to influence cell
proliferation, differentiation and apoptosis
◦ Omega-3 fatty acids can repress this inflammation
◦ In healthy adults, the distal part of the gastrointestinal tract is characterized
by a low level of oxygen tension as oxygen is used in epithelial cells for
oxidative phosphorylation in the mitochondria. The colon usually harbors large
communities of obligate anaerobes.
◦ In patients with Inflammatory Bowel Disease (IBD), fewer species of the
obligate anaerobes, phylum Firmicutes were present in IBD patients.
◦ The changing oxygen conditions may be due to the inflammatory reaction
itself, causing an oxidative burst in the intestinal tissue, for example, by the
release of reactive oxygen species by neutrophils.
◦
◦ Rigottier-Gois L. Dysbiosis in inflammatory bowel diseases: the oxygen hypothesis. ISME J. 2013;7(7):1256–1261
◦ Recent work suggests that anaerobiosis in the colon is maintained by
colonic epithelial cells (colonocytes), which consume oxygen through
oxidative phosphorylation in their mitochondria, thereby maintaining the
epithelial surface in a state of physiological hypoxia.
◦ By increasing epithelial oxygenation, colitis drives an aerobic expansion of
colibactin-producing E. coli, and Proteobacteria in the colon, also observed for other conditions that are associated with an increased risk for colorectal cancer formation, including a high-fat diet, antibiotic treatment, and alcohol dependence.
◦ Bacteria-derived butyrate affects colon epithelial O2 consumption
and results in stabilization of hypoxia-inducible factor (HIF), a
transcription factor coordinating barrier protection that requires SIRTNAD+
for activation.
◦ 3 days of Abx administered by oral gavage resulted in a nearly
complete loss of bacterial groups. Despite outgrowth of several
resistant organisms, cecal contents from abx-treated mice lost the
ability to produce SCFAs from inulin and lost HIF expression, both of
which are restored by butyrate administration.
◦ Metabolism of butyrate by epithelial cell lines depletes local
O2 (being used in oxidative phosphorylation in epithelial cell
mitochondria) to the extent that HIF is stabilized.
◦ Interestingly, mice with mitochondrial polymorphisms that maintain
increased oxidative phosphorylation activity are resistant to colitis.
◦ The primary energy source for cancerous colonocytes is glucose
(Warburg effect)
◦ Activated AMPK is an endogenous inhibitor of the Warburg effect
◦ Butyrate is a potent activator of AMPK in colonic cell lines
The Microbiome and the Circadian Rhythm
◦ Intestinal microbiota generates diurnal rhythms in innate immunity that synchronize with feeding rhythms to anticipate microbial exposure.
◦ Rhythmic expression of antimicrobial proteins was driven by daily rhythms in epithelial attachment by segmented filamentous bacteria (SFB), members of the mouse intestinal microbiota.
◦ Mechanistically, rhythmic SFB attachment activated an immunological circuit involving group 3 innate lymphoid cells. This circuit triggered oscillations in epithelial STAT3 expression and activation that produced rhythmic antimicrobial protein expression and caused resistance to Salmonella Typhimurium infection to vary across the day-night cycle.
◦ Host feeding rhythms synchronize with the microbiota to promote rhythms in intestinal innate immunity that anticipate exogenous microbial exposure.
Bile acids
Bile acids are detergents derived from cholesterol that aid in digestion and nutrient absorption
Hormone-like signaling agents between gut-liver-brain involved in glucose, lipid, and energy metabolism/homeostasis
Bactericidal modulation of the microbiome
Regulate mucosal homeostasis and inflammation
Promote hematopoietic stem cell expansion in the fetal liver
Gut microbes influence the composition of the circulating bile acid pool to prevent bactericidal activity and digestion of self
Conjugated to taurine/glycine to retain structure critical for lipid emulsifying activities in the acidic duodenum
Secondary BAs, inflammation and cancer
Derivatives of primary bile acids generated by microbial metabolism in the intestine. (Chen, 2019)
DCA and LCA promote cell cycle arrest and apoptosis primarily through the generation of intracellular reactive oxygen species (ROS), genomic DNA breakage, activation of inflammasome.
DCA suppresses p53 in response to DNA damage (senescence), activates resistance to apoptosis, angiogenesis (prostaglandin E2 through vascular endothelial growth factor), activates proliferation
and oxidative stress.
In response to repeated DNA damage due to the exposure of secondary BAs, the large number of cell generations in the colonic (and other gastrointestinal) epithelia may allow time for induction and
selection of mutations leading to cancer in humans
Bile acids and the brain
Activate bile acid receptors in the blood brain barrier (BBB) and brain to regulate neuroinflammation and neurodegeneration (Ferrell, 2021, Chen, 2019)
Increased secondary BAs (DCA, LCA) in serum of Alzheimer’s Disease (AD) patients, worsening from MCI to AD and worsening ratio of DCA:CA indicating bacterial dihydroxylation
Multiple bile acid receptors (CAR, PXR, FXR, S1pr2, TGR5) present on neurons, microglia, astrocytes
Suggests protective effects via TGR5 and potentially detrimental effects via FXR and S1pr2
Tryptophan metabolism
Most ingested protein is digested and
absorbed in the small intestine
Significant amounts of proteins and
amino acids (6–18 g/day) may reach
the colon
Endogenous tryptophan conversion to
metabolites: kynurenine, kynurenic
acid, xanthurenic acid, and
cinnabarinic acid, NAD+
Kynurenine pathway
Goal of making NAD+ for energy for astrocytes and microglia
Indoleamine 2,3-dioxygenase (IDO) enzyme triggered by pathogens and cytokines like TNFa
Quinolinic acid (QA), an intermediary in the kynurenine pathway, is activating and toxic to the
CNS.
stimulates astrocytosis
is excitotoxic to neurons via the NMDAR
can induce apoptosis in astrocytes, neurons, and oligodendrocytes.
Kynurenine also has vasoactive effects
exacerbate CNS infection and inflammation
through pericytes kynurenine production disrupts the integrity of the BBB
Tryptophan metabolism
Also in the colon, bacterial protein catabolism increases with increased protein intake,
carbohydrate depletion in the colon, increased colonic pH and prolonged colonic transit
time
In 1897, tryptophan was found to be converted into indole by Bacillus coli (now Escherichia
coli)
Tryptophan is one of the nine essential amino acids, which the human organism cannot
synthesize, and which therefore must be supplied in the diet.
Indole is well-described as an intercellular signal molecule that appears to be important in
microbial communities by affecting spore formation, drug resistance, biofilm formation, and
virulence
Indole strengthens the gut mucosal barrier and mucin generation; increases IL-10 expression
and reduces inflammatory indicators
Tryptamine, a tryptophan catabolite produced by C. sporogenes and Ruminococcus gnavus induces the release of the neurotransmitter serotonin by enterochromaffin cells. Serotonin
stimulates gastrointestinal motility by acting on enteric nervous system neurons
3-indoxyl sulfate (IS) is a tryptophan metabolite, uremic toxin which correlates with the development of CKD and cardiovascular disease; urinary IS level is a common marker of intestinal dysbiosis
Fiber
Plant-derived nonstarch polysaccharides, resistant oligosaccharides, lignin, and resistant starch
Water solubility within the gastrointestinal tract is related to the degree of fermentation by gut microbes. Soluble dietary fibers can increase digesta viscosity, which in turn delays gastric
emptying and nutrient release, thus reducing glycemic response.
Fermented in the colon by the microbiome to SCFAs
Production of SCFAs differs by microbial composition of the gut microbiome
Improvements in inflammatory conditions such as cardiovascular disease, type 2 diabetes, metabolic syndrome, and depression have been linked to high intakes of dietary fiber.
High dietary fiber intake has been associated with lower levels of CRP, leptin, and higher adiponectin
Dietary fiber and allergy
Dietary fiber intake significantly suppressed the allergic responses, attenuated allergic symptoms of nasal rubbing and sneezing
Decreased the pathology of eosinophil infiltration and goblet cell metaplasia in the nasal mucosa and lung, inhibited serum OVA-specific IgE levels, and lowered the levels of Th2 cytokines in NALF and BALF, but increased Th1 (IFN-γ) cytokines.
Also increased the proportion of Bacteroidetes and Actinobacteria, and decreased Firmicutes and Proteobacteria. Levels of probiotic bacteria, such as Lactobacillus and Bifidobacterium, were upgraded significantly.
Fasting; its all about the ketones
Energy restriction for 10 to 14 hours or more results in depletion of liver, brain glycogen stores
and hydrolysis of triglycerides (TGs) to free fatty acids (FFAs) in adipocytes. FFAs released into
the circulation are transported into hepatocytes, where they produce the ketone bodies
acetoacetate and β-hydroxybutyrate (β-HB).
The metabolic switch from the use of glucose as a fuel source to the use of fatty acids and
ketone bodies results in a reduced respiratory-exchange ratio (the ratio of carbon dioxide
produced to oxygen consumed), indicating the greater metabolic flexibility and efficiency of
energy production
Cells respond to intermittent fasting by engaging in a coordinated adaptive stress response
that leads to increased expression of antioxidant defenses, DNA repair, protein quality control,
mitochondrial biogenesis and autophagy, and down-regulation of inflammation
Fasting/ketogenesis
Ketone bodies are potent signaling molecules that regulate the expression and activity of
many proteins and molecules known to influence health and aging.
Ketone bodies stimulate expression of the gene for brain-derived neurotrophic factor (BDNF),
with implications for brain health and psychiatric and neurodegenerative disorders.
Reduced levels of glucose and amino acids during fasting result in reduced activity of the
mTOR pathway and up-regulation of autophagy.
Glycolysis in cytoplasm

oxidative phosphorylation

energy yield

beta oxidation
osteoarthritis inflam

inflammasome

senescence
microbiome

PAMPs and DAMPs


bile

tryptophan

Sleep
Circadian rhythm endogenously generated by suprachiasmic nucleus in the hypothalamus in
response to photic signals and non-photic signals (food, social interaction, and locomotor
activity), requires NAD+
In humans, circadian misalignment can occur with shift work, jet lag, chronic sleep loss
Can contribute to the pathophysiology of metabolic syndrome, liver disease, cancer,
cardiovascular disease, neurodegenerative disease and mood disorders.
Bile acid homeostasis is regulated by circadian rhythm, altering Cyp7a1 gene expression
Chronic circadian disruption leads to global deregulation of lipid and bile acid pathways
Unconjugated bile acids, generated by gut microbes alter the expression of CLOCK genes.
Sleep and inflammation
Subjective sleep quality [assessed with the National Institutes of Health Patient-Reported
Outcome Measurement Information System (PROMIS)], was inversely correlated with CRP
levels in well-phenotyped IBD patients.
Wilson,. “High C-Reactive Protein Is Associated with Poor Sleep Quality Independent of Nocturnal Symptoms in Patients with Inflammatory Bowel
Disease.” Digestive Diseases and Sciences 60, no. 7 (July 1, 2015): 2136–43.
In a prospective cohort, anti-inflammatory therapies with anti-integrin (vedolizumab) and anti-
TNF agents (infliximab or adalimumab) resulted in improved sleep quality (assessed with
PROMIS) within 6 wk of therapy initiation
Sleep dosing
Sleep variability, social jetlag, and later sleep timing were associated with adverse health outcomes
Weekend catch-up sleep was associated with positive health outcomes
Chaput, J. “Sleep Timing, Sleep Consistency, and Health in Adults: A Systematic Review.” Applied Physiology, Nutrition, and
Metabolism 45, no. 10 (Suppl. 2) (October 1, 2020): S232–47.
Based on data from the Nurses’ Heath Survey with over 400 IBD cases, self-reported sleep duration of
<6 h and >9 h per night increased risk of ulcerative colitis
Ananthakrishnan,. “Sleep Duration Affects Risk for Ulcerative Colitis: A Prospective Cohort Study.” Clinical Gastroenterology
and Hepatology 12, no. 11 (November 1, 2014): 1879–86.
Sleep disturbance was associated with higher levels of CRP (ES 0.12; 95% CI 0.05 – 0.19) and IL-
6 (ES 0.20; 95% CI 0.08 – 0.31). Shorter sleep duration, but not the extreme of short sleep, was
associated with higher levels of CRP. reference category for sleep duration was 7–8 h per
night in the majority of studies.
Butyrate
A short chain fatty acid (SCFA) produced by obligate anaerobes fed insoluble fiber
The preferred fuel source for intestinal epithelial cells
Promotes an antibacterial activity in intestinal macrophages (Marizzoni, 2020)
Restricts bacterial translocation
A histone deacetylase inhibitor
Transcriptional modulator
Anti-inflammatory molecule on microvascularity
Decreases the endothelial Nlrp3 inflammasome assembly and IL1 production formation
and activation in endothelial cells. (Ferrell, 2021)
Also produced by the liver in response to fasting (R-BHB) (Bradshaw, 2020)
Butyrate and inflammation
Dampens systemic immunity and CNS glia activity.
Induces the melatonergic pathway, allowing it to have mitochondria optimizing effects.
Increases the cytotoxicity of natural killer cells, which are the cells that the body uses to deal with cancers and viruses
Exogenous ketone bodies (R-BHB) stimulate a program of gene expression
that alters metabolism to restore cellular redox function through the
restoration of the coenzyme ratios that largely control metabolic flux
through central metabolic pathways.
Ketone ester was able to decrease chromosomal damage in mice and
increase survival in cells exposed to ionizing radiation
Low dose naltrexone
Opioid known to modulate mu, k and d opioid receptor (MOR) responses
Opioid inactive (+)-isomers of Naltrexone inhibit lipopolysaccharide-induced Toll
like Receptor 4 (TLR4) signaling
Wound healing of intestinal epithelial barriers is modulated by improved migration
rather than proliferation (Lie, 2018)
Attenuate the production of proinflammatory cytokines and neurotoxic superoxides
via suppressive effects on central nervous system microglia cells (Younger, 2014)
Neuroprotective effects via modulation of mitochondrial apoptotic pathways (San- Emeterio, 2006)
Treating with LDN
Potential SE: vivid dreams, drowsiness, headache
Vivid dreams resolve with alternate morning dosing
Studies above use 4.5mg caps nightly
Specialized Pro-resolving Mediators
Resolvins, protectins, and maresins: bioactive metabolomes that each stimulate self-limited innate responses, enhance innate microbial killing and clearance, and are organ-protective.
Biosynthesized from eicosapentaenoic acid (EPA), docosapentaenoic acid (n-3DPA), or docosahexaenoic acid (DHA)
Not immunosuppressive, but rather new immunoresolvent
Counterregulate proinflammatories and actively promote resolution via monocyte/macrophage uptake of debris, apoptotic PMNs, and killing/clearing microbes and efferocytosis of apoptotic
granulocytes
Downregulates leukocyte adhesive molecules and platelet activation
Enhanced in hypoxia, reduces dendritic cells’ IL-12 production, potently stimulate IL-10 and
phagocytosis
Clinically,
attenuates contact hypersensitivity in skin,
Cardioprotective, protects from PMN-mediated reperfusion organ injury
Potent neuroprotective actions in retina, brain, and pain
Treating with SPMs
Omega 3 FAs, cold water fish like salmon
Strenuous exercise
Buckley, Christopher D., Derek W. Gilroy, and Charles N. Serhan. “Pro-Resolving Lipid Mediators and Mechanisms
in the Resolution of Acute Inflammation.” Immunity 40, no. 3 (March 20, 2014): 315–27.
Active fractionated marine lipid concentrate 300mg-3g
T/UDCA
Naturally-occurring hydrophilic bile acid that has been used for centuries in traditional Chinese medicine (TCM).
The taurine conjugate of ursodeoxycholic acid (UDCA), a secondary bile acid that can be produced exclusively by intestinal microbiota
Food and Drug Administration (FDA) for treatment of primary biliary cholangitis
Potential therapeutic benefits in diabetes, obesity, and neurodegenerative diseases, mostly due to its
cytoprotective effect.
MOA: alleviation of (ER) stress and stabilization of proteins for correct folding and prevention of
aggregation, a chemical chaperone, .
Reduce oxidative stress, suppress apoptosis, and decrease inflammation in many in-vitro and in-vivo models
and in humans with various diseases.
Inflammation as a Cause of IR
• Excessive production of inflammatory compounds
in the body can cause IR
• Inflammatory substances damage and/or
inactivate insulin receptors.
• Contributes to breakdown of one or more factors
needed to complete the process of glucose
transport
• IR leads to ↑ inflammatory markers
• Including ferritin, uric acid, white cell counts, fibrinogen, CRP and
IL-6
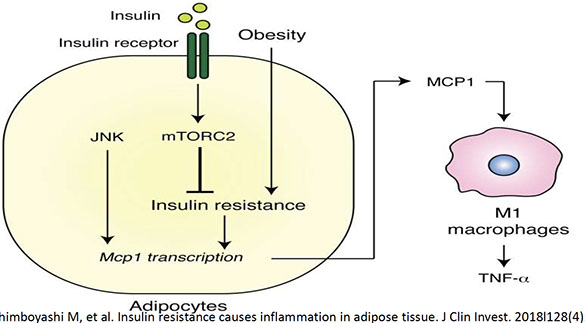
• insulin resistance in adipocytes results in production of the
chemokine monocyte chemoattractant protein 1 (MCP1)
• This recruits monocytes and activates proinflammatory
macrophage
• Insulin resistance is correlated with reduced insulin/mTORC2
signaling and elevated MCP1 production in visceral adipose tissue
T2D Inflammation
• T2D is an inflammatory disease
• T2DM promotes increased levels of pro-inflammatory cytokines including
TNFα and IL-6
• Involved in the development of insulin resistance in skeletal muscle
• Studies report inflammatory pathways in muscle - in particular, NF-κB -
contributes to T2DM-mediated muscle atrophy
• 2016 cohort of obese patients with T2DM compared to age-matched
controls
• Demonstrated patients with T2DM have 60% higher skeletal muscle
expression of the atrophy transcription factor FoxO1
Adiponectin and Mitochondria
• Adiponectin is an anti-diabetic adipokine
• Mitochondrial function linked to adiponectin synthesis
in adipocytes
• Mitochondrial dysfunction increased with excess
adipose tissue
• Decreases plasma adiponectin levels
• Adiponectin induces Ca++ influx via receptor
• AdipoR1 = adiponectin receptor
• Suppression of AdipoR1 results in decreased PGC-1α
• Leads to decreased mitochondrial content
• Decreased blood glucose control
GLUT 4 Glucose Transporter
• Glucose transporter type 4 - Hexose transporter system
• Uses ATP-independent, facilitative diffusion mechanism
• Mediates insulin-stimulated glucose transport in fat and muscle
• Predominantly expressed in skeletal muscle and adipocytes
• Failure of GLUT4 to translocate to the plasma membrane in response to insulin
• An early step in the development of insulin resistance and type 2 diabetes
Glut 1 Dominated Transport
• Leads to Increase RNA, DNA, NAD + FAD
• Increases the Pentose Pathway
• Regenerates its own glutathione (NADPH)
• GLUCOSE THROUGHPUT
• LACTATE PRODUCTION
• Intracellular pH reduced H+ ions pumped into intracellular space
creating necrotic space
adiponectin

Neuroinflammation
Inflammation of Central Nervous System (CNS) tissue
Mild inflammation – beneficial; CNS’ natural defense
Chronic inflammation - a BIG problem
Leads eventually to:
Neuronal Dysfunction
Neuronal Injury
Neuronal Death
Causes of
Neuroinflammation
Traumatic brain injury (TBI)
Sports and Recreational injuries
Military
Motor vehicle accidents
Electric shock/lightening strikes
Violence
Immune/autoimmune conditions
Neuronal Degradation
Aging
Chronic stress
ECM: Governs Cellular Functions
● Cocktail of proteins, signalling
molecules, and chemicals that
cells exude as they grow
● Cells use matrix to impart
strength & shape to tissues like
bone & brain
● ECM used to be dismissed as
an inert garden trellis, now
proven that ECM is critical for
cell behavior
● Muscle stem cells self renew only
on soft gels (not hard plastic
plates)
● ECM guides stem cells to
repair damaged tissues, reform
blood vessels damaged
by stroke & alter cellular
responses to chemotherapy
● ECM serves as a reservoir of
signaling molecules that
serves as a highway between
cells
● (25 yrs ago, ECM was just
thought to be structural)
● Regen med is trying to
improve engineered ECMs but
can be tricky
● Each synthetic or naturally
derived biomaterial has pros
and cons
Aromatase Inhibitors Musculoskeletal Syndrome (AIMSS)
● AIMSS is characterized by joint stiffness, decreased grip strength,
arthralgia, and myalgia likely caused by tenosynovial changes and intraarticular
fluid retention (25).
● Postmenopausal women taking AIs experience vaginal dryness and
sexual dysfunction compared to postmenopausal women without
breast cancer (26).
● Post-menopausal women have fewer relaxin and estrogen receptors on
fascial fibroblasts implying that postmenopausal women have fascia
that will not respond to usual hormonal cues (4).
● These hormonal cues prompt elastin synthesis; without elastin, these
women experience body stiffness.
fascia



Labs
Assessing Metaflammation ‐ Basic LABS
• Cortisol serum
• CRP‐hs
• MPV
• Vitamin D total
• IL‐6
• Homocysteine
• B12/RBC folate
• Monocytes/Baso/Eosin %
• WBC’s
• oxLDL
• Galectin‐3
• Platelets
• Fibrinogen
• 8‐OHdG
• F2 isoprostane
• Iron, total
• TIBC
• % Saturation
• Ferritin
• VEGF
• TGF‐beta1
• Adiponectin/Leptin
• MMP‐9
• GlycA
• Neopterin
• Histamine
• Zonulin
• Anti‐parietal cell antibodies
• LDH
• Uric acid
Genetic Variants in MetS
• 2019 cross sectional study, n=224 MetS cases and 200 control
• Fasting bloodwork measured
– Serum glucose, insulin, lipid profile, interleukin‐6 (IL‐6) and tumor necrosis factor α (TNF‐α)
• Genetic variants of IL‐6, TNF‐alpha and insulin resistance much higher than controls
• IL‐6 positive correlation w/ HOMA‐IR and TNF‐alpha
• CC genotype of IL‐6 was associated with the increased risk of MetS
• Serum TNF‐alph and IL‐6 significantly higher in AA and
CC genotypes of TNF‐alpha/IL‐6 as compared to GG
Pharmacy types
503-A
Traditional compounding pharmacy
• USP <795> and <797> guidelines
• Patient specific prescriptions
– No office use
• Smaller batches
– Limited to anticipatory compounding (30
days)
• Largely regulated by state boards of
pharmacy
– FDA Influence
• May be compounded from FDA approved
finished product or bulk drug substance if
certain provisions are followed
comply with an applicable United States
Pharmacopeia (USP) or National Formulary
(NF) monograph if one exists, and the USP
chapter on pharmacy compounding;
• are components of FDA-approved drug
products if an applicable USP or NF
monograph does not exist; or
• appear on FDA’s list of bulk drug
substances that can be used in
compounding (the 503A bulks list) if such a
monograph does not exist and the
substance is not a component of an FDAapproved
drug product.
Category 1 – These substances may be eligible for inclusion on the list of bulk
drug substances that can be used in compounding under section 503A, were
nominated with sufficient information for FDA to evaluate them, and do not
appear on any other list. FDA does not intend to take action against a
compounder for compounding drugs using bulk drug substances listed in
Category 1, provided that the conditions described in the guidance document
are met.
• Category 2 – These are bulk drug substances that were nominated with
sufficient supporting information for FDA to evaluate them and they may be
eligible for inclusion on the 503A bulks list. However, FDA has identified
significant safety risks relating to the use of these substances in compounding,
and therefore, pending further evaluation, drug products compounded using
these substances are not eligible for the policy described for the substances in
Category 1. FDA would consider taking action against a compounder for
compounding drug products with this bulk drug substance under its general
enforcement policies. See Safety Risks Associated with Certain Bulk Drug
Substances Nominated for Use in Compounding for the substances and a
summary of the identified safety risks.
• Category 3 – These substances may be eligible for inclusion on the 503A bulks
list, but were nominated without sufficient supporting information for FDA to
evaluate them. These substances are not eligible for the policy that applies to
substances in Category 1. FDA would consider taking action against a
compounder for compounding drug products with this bulk drug substance
under its general enforcement policies. These substances can be re-nominated
with sufficient supporting information through Bulk Drug Substances That Can
Be Used To Compound Drug Products in Accordance With Section 503A of the
Federal Food, Drug, and Cosmetic Act; Establishment of a Public Docket.
503-B
Current good manufacturing practices (CGMP)
• 21 CFR Part 210 and 211
• Regulated by FDA
– States are beginning to enact their own
503B laws
• May compound for office use
• May compound in larger batches
• All processes, equipment, and facilities
must be validated
• Stability indicating studies required for
products
• May be compounded from FDA approved
finished product or bulk drug substance if
certain provisions are followed
the bulk drug substance appears on a
list identifying bulk drug substances
for which there is a clinical need
(the 503B bulks list), or
• the drug product compounded from
such bulk drug substance appears
on FDA’s drug shortage list at the
time of compounding, distribution
and dispensing.
Category 1 – These substances may be eligible for inclusion on the 503B bulks
list, were nominated with sufficient information for FDA to evaluate them, and
do not appear on any other list. FDA does not intend to take action against an
outsourcing facility for compounding drugs using bulk drug substances
identified in Category 1 provided that the conditions described in the guidance
document are met.
• Category 2 – These are bulk drug substances that were nominated with
sufficient supporting information for FDA to evaluate them, but FDA has
identified significant safety risks relating to the use of these substances in
compounding pending further evaluation. Drug products compounded using
these substances are not eligible for the policy described for the substances in
Category 1. FDA would consider taking action against an outsourcing facility
for compounding drug products with this bulk drug substance under its
general enforcement policies. See Safety Risks Associated with Certain Bulk
Drug Substances Nominated for Use in Compounding for the substances and a
summary of the identified safety risks.
• Category 3 – These substances may be eligible for inclusion on the 503B bulks
list, but were nominated with insufficient supporting information for FDA to
evaluate them. The substances are not eligible for the policy that applies to
substances in Category 1. FDA would consider taking action against an
outsourcing facility for compounding drug products with this bulk drug
substance under its general enforcement policies. These bulk drug substances
can be re-nominated with sufficient supporting information through Bulk Drug
Substances That Can Be Used To Compound Drug Products in Accordance With
Section 503B of the Federal Food, Drug, and Cosmetic Act; Establishment of a
Public Docket.

Peptides
ACE‐031
• Fusion peptide of activin receptor type IIB and IgG1‐Fc
• Binds myostatin and related ligands
• Myostatin inhibitor
• Used in humans for Duchenne Muscular dystrophy
– Reported to disrupt the inhibitory effect on muscle
development
– No adverse events in 2017 randomized, double‐blind placebocontrolled
ascending dose trial
• Also noticed in these study patients:
– Improved maintenance of the 6‐minute walk test (6MWT)
distance
– Trend for increased lean body mass and bone mineral density
(BMD)
– Reduced fat mass
– Dosage = 0.5 – 2.0 mg/kg Q2 weeks x 3 months
• Safety in human studies:
– Most common issue = injection site erythema (20.8%)
– Telangiectasia (20.8%)
– Epistaxis (16.7%)
– Erythema (12.5%)
– Headache (12.5%)
• No subjects discontinued treatment
Aged Garlic Extract
• Special garlic extract – higher levels of S-allyl cysteine vs.
regular garlic
• Proprietary Aging Process 20 months
• Removes volatile compounds and produces NEW watersoluble
compounds
• Not BLACK GARLIC
• Over 900 clinical studies supporting uses – human and lab
• Decreases LDL(and OxLDL) cholesterol while improving HDL
• Decreases metaflammation(IL6, TNF alpha)
• Effects against atherosclerosis development
• Inhibits coronary artery calcification (incl vulnerable plaque)
• Lowers homocysteine – improves methylation
• Microbiome supportive
• Neuroprotective
Aged Garlic Extract and IL-6, TNF-alpha
• Supports cardiovascular health, blood pressure, nitric oxide
• Reduces low attenuation plaque in coronary arteries
• Supports immunity - enhances immune cell function –
• NK cells, decreases Il-6 and TNF-alpha
• Antiviral activity
• Excellent antioxidant
• Improves blood pressure – approx. 16%
Aged Garlic Extract Immunity
• AGE reported to modulate inflammation and immunity - especially
those with obesity
• Clinical study n=51 adults with obesity, age 45.6 + 1.6yr
• Randomized, parallel, double-blind, placebo-controlled study for 6
weeks
• AGE 3.6gm daily or placebo
• Il-6 and TNF-alpha significantly lower in AGE
• LDL lower also in AGE individuals
New Research - AGE and Reducing Chronic
Inflammation
• 2019 double-blind, placebo controlled randomized clinical study
• n= 51 healthy but obese adults
• 3.6gm AGE daily in divided doses x 6wk
• IL-6 and TNF-alpha significantly lower in AGE vs. placebo
• Increased gamma-delta T cells – modulated immunity
• Significant reduction in LDL cholesterol
AGE Reduces Plaque in Coronary Arteries
• Single-center, randomized, placebo-controlled, double-blind trial at Harbor UCLA Medical
Center
• Published in Feb. 2020 Experimental and Therapeutic Medicine
• n= 66 final patients with diabetes mellitus
• 30-75 years, HbA1c>6.5%, Fasting blood glucose>125mg/dl)
• 2,400mg AGE or placebo x 12 months
• RESULTS:
• AGE suppresses adverse cardiovascular events by reducing low-attenuation plaque,
decreasing left ventricular mass and improving endothelial function
New Research - Aged Garlic Extract Improves
Microcirculation
• 2019 double-blind, placebo-controlled study
• N= 93 patients aged 40-75 w/ Framingham Risk Score > 10, CAC score > 10
completed test
• 2,400mg AGE daily for 12 months
• RESULTS:
• ★ AGE suppresses adverse cardiovascular events by reducing CAC progression in
not only non-Europeans but also European population
• ★ AGE facilitates wound healing by increasing the level of microvascular blood
flow
General dosage - 1-2 caps 2 times daily (600-1,200mg)
• New caplet = 2,400mg AGE daily ( a cap TID)
• Adds Grape seed extract 95% 300mg/ day for added vascular and BP support
• Immune and inflammation support; MetS support = 3.6 gm daily in divided
doses
• Does NOT interact with anticoagulants unlike other garlic preparations
Alpha GPC
• L-Alpha glycerylphosphorylcholine
• Natural choline compound
• Crosses BBB readily
• Improves mitochondrial function
• Supports growth hormone levels
• 300-600mg BID
ALA
• Affects beta cell function
• ↑cAMP-activated protein kinase (AMPK)
• ↑ PGC-1 alpha, ↑ PPAR alpha
• Improves glucose utilization and mitochondrial biogenesis
• Studies report exercise and ALA therapy improves IRS-1 dependent insulin
signaling
• DOSE = 600mg BID
• Nephroprotective
• Detoxifies heavy metals
ALRN‐5281 Peptide
• GHRH agonist – long‐acting growth hormone releasing
hormone
• Clinical studies on this peptide by Alieron
Therapeutics
• Used for treating:
– Orphan endocrine disorders
– Adult growth hormone deficiency
– HIV lipodystrophy
– Broader patient populations – metabolic/endocrine disorders
– Performance enhancement
• Initial Phase 1 trial evaluated the safety and tolerability of
single ascending doses of SubQ ALRN‐5281 in 32 healthy
adult subjects
• No serious adverse events, dose‐limiting safety findings, or
tolerability issues leading to withdrawal during the study
• Dosing
– 0.05 – 0.15 mg/kg subQ once weekly
ARA-290
• Non-erythropoietic/hematopoietic 11 amino acid peptide
• Also called helix B surface peptide (HBSP)
• Designed from structure of erythropoietin - preserves health effects
of EPO w/out creating RBCs
• Improves metabolic control
• Anti-inflammatory, anti-apoptic, anti-permeability effects
• Improves neuropathic symptoms in T2D patients
• Inhibits vascular leakage
• Protects against neuroglial degeneration
• Analgesic effect of ARA-290 is mediated by its anti-inflammatory and
immunomodulatory functions
• Inhibits TNF-alpha, NF-kB
• Targets the innate repair receptor (IRR) to down-regulate
inflammation to alleviate neuropathic pain
• Lab studies report ARA 290 inhibits TRPV1 channel activity
• Relieved the mechanical hypersensitivity induced by capsaicin
• Leads to decreased neuropathic pain
• Cibinetide is trade name – Araim Pharmaceuticals
• Granted US and EU Orphan Drug Designation for the treatment of
sarcoidosis
• US Orphan Drug Designation for treatment to increase survival and
improve functioning of pancreatic islets following transplantation.
• Improves Engraftment in Pancreatic Islet Transplantation by:
• Protecting Islets
• Reducing Inflammatory Reactions
Suggested Dosage :
• 6mg/ml 4ml vial
• 4mg (0.67ml) SubQ three times per WEEK x 4-5 weeks
AT-1001
larazotide
Larazotide is a novel, locally acting, non-systemic, synthetic 8-
amino acid oral peptide, discovered during functional
screening of synthetic Vibrio cholera related peptides.
Larazotide acetate is a first-in-class tight junction (TJ) regulator
Larazotide prevents opening of intestinal TJs by promoting TJ
assembly and actin filament rearrangement, which prevents
gluten/gliaden and pathogens from reaching the intestinal
submucosa and triggering an inflammatory response,
macrophage recruitment and increases in intestinal
permeability (Hoilat 2021)
type 1 diabetes, other autoimmune diseases, inflammatory
bowel disease, Kawasaki disease, respiratory (infective and/or
non-infective) diseases.
Jacopo, T. “The Therapeutic Use of the Zonulin Inhibitor AT-1001 (Larazotide) for a
Variety of Acute and Chronic Inflammatory Diseases.” Current Medicinal Chemistry 28
(December 31, 1969): 1–20.
Larazotide prevented gluten-induced symptoms and
blunted increases in anti-tTG antibodies, INF-gamma, and
intestinal permeability
Safety profile comparable to placebo
BAM-15
• On horizon
• Mitochondrially targeted small molecule - mitochondrial uncoupler
• Enhances mitochondrial respiratory kinetics
• Improves insulin action
• Stimulates nutrient uptake by sustained activation of AMPK
• Therapeutic potential for treating obesity and associated
comorbidities
Benfotiamine
• Lipid soluble form of vitamin B1 (thiamin)
• Improves carbohydrate and amino acid metabolism to produce
cellular energy.
• Helps improve glucose regulation and insulin sensitivity
• Dose 100-150mg/day
• Clinical studies in diabetics report benfotiamine:
• Helps prevent endothelial dysfunction
• Decreases advanced glycation end-products (AGE)
• Decreases markers of inflammation
• Improves diabetic retinopathy symptoms
Beta 1,3 – 1,6 glucan Oromucosal Nanospray
• “SMART” Formulation of low molecular weight beta-glucans
• Extracted from the Almond Mushroom (Agaricus blazei)
• High levels of beta-1,3-1,6 glucan and zinc
• Sustainable cultivation in Brazil
• Oromucosal spray = most bioavailable oral beta-glucan supplement on market
• Beta-1,3-1,6 glucans reported in human trials to:
• Decrease metainflammation – improve inflammatory biomarkers
• Immune modulators
• Improve innate immune response
• Decreased infections
• Reduction of colds/flu symptoms + days sick
• Fewer URTI symptoms
• “TRAINS” T cells for more effective immune response – memory improved
• Bind to Dectin-1 domains on immune cells
• Increases dectin-1 CR3 signaling (complement receptor)
• Enhances oxidative bursts from primed innate immune cells
GENERAL IMMUNE SUPPORT
• A puff in the left and right inner cheek (buccally) and
under the tongue (sublingually) – 3 sprays
• Wait for 10 seconds and then swallow
• This sequence should be performed 3 times – 9 puffs total
• Repeat the whole procedure 3x daily - in the morning, noon and evening - before
meals and after brushing teeth
• Total of 27 puffs per day = 132mg highly absorbable nanotized beta 1,3-1,6
glucans
• In acute needs, dosage frequency may be increased
• May be used topically
BPC-157
(0ral) (Cellular repair)- overall inflammation, improves immune strength and gut
health, improves energy and optimizes growth hormone receptors, anti-inflammatory,
immune strengthening
(cellular repair)- decreases inflammation, increases collagen synthesis, quicker
recovery times post-injury, wound and bone healing
15aa active fragment of naturally-occurring BPC
A crucial organoprotective mediator of the stomach stress coping response
disovered in 1990 in Croatia
Sikirić, P. “A New Gastric Juice Peptide, BPC. An Overview of the Stomach-Stress-Organoprotection Hypothesis and Beneficial Effects of BPC.” Journal of Physiology-Paris 87, no. 5 (January 1993): 313–27.
A free radical scavenger to counteract reperfusion-induced oxidative injury
A membrane stabilizer, counteracting leaky gut syndrome by modulating ischemiainduced increased capillary permeability
Dosage range of BPC most employed in animals has been between 10
mcg and 10 ng/kg ip, ig, iv or topical. In some studies, however, even lower
dosages were effectively used
No LD
Bovine Colostrum
• Supplies protein, immune factors, growth factors vitamins,
minerals
• Rich in iron-binding proteins (lactoferrin and lactoglobin)
• Natural source of IgA, IgD, IgE, IgG, IgM
• Supports immunity and cytokine system
• Supports GUT health to prevent dysbiosis
• DOSE 10,000 mg daily

CB4211 Peptide
• Mitochondrial peptide
• Derivative of MOTS‐c
• Useful in obesity/ fatty liver
• Reported to enhanced insulin mediated phosphorylation of IR,
IRS‐1, and Akt, without affecting IGF mediated
phosphorylation of IGF‐1R
• Consistent with activity through IR, CB4211 potentiated
insulin induced reduction in glucose production in H4‐IIE cells
• Animal Studies
– Reported to reduce NAFLD activity score, markers of
livery injury, body weight, and fat mass in animal
models of NASH or obesity
– lab mice with insulin enhanced insulin sensitivity,
prolonging the reduction in blood glucose levels
compared to insulin alone
• Human Study
– Phase 1b randomized, double‐blind placebo‐controlled
study using CB4211 25mg once daily x 4 weeks in
obese subjects w/ NAFLD
Loomba R, et al. AASLD Poster LB5. CB4211, a Novel Analog of MOTS‐c, Improves Markers of Liver Injury and
Metabolism in Obese Subjects with Nonalcoholic Fatty Liver Disease: a Multicenter, Double‐Blind, Randomized,
Placebo‐Controlled Study.
• Results:
– CB4211 well tolerated and safe
– No serious adverse events
– Robust reduction of:
ALT (‐21%)
AST (‐28%)
Glucose (‐6%)
– Lowered body weight
– Lowered liver fat content
• Human Dosage:
– 25mg SubQ x 4 weeks
Chondroitin Sulfate
• Dosage: 600mg, 3 times a day, with meals. For maintenance 300mg, 2-3 times per
day, with meals
• Synergistic effect with glucosamine
• Active Forms: Chondroitin sulfate (CS), as chondroitin-4-sulphate and
chondroitin-6-sulphate, found naturally combined with Type II collagen
• Stimulate proteoglycan production
• Inhibits breakdown or destruction of connective tissue matrix
Chromium
• Important in insulin regulation and blood sugar control
• Metabolism of carbs and fats
• Improves satiety
• ↓Carbohydrate cravings
• Helps convert T4 to T3
• Chromium depleted in high sugar diets
• Dosing 800mcg-1600mcg/day GTF chromium
Cistanche sp.
• “Desert ginseng”
• Used in Traditional Chinese Medicine
• Neuroprotective; decreases microglial activation
• Immune supportive
• Activates caspase-3 and caspase-8
• Helps improve mitochondrial function
• Improves cognitive function
• Dosage = 200-300mg daily
• Standardized to 22% echinacosides
CoQ10
CoQ10 Drug-Induced Nutrient Depletion
DIND
• HMG-CoA reductase inhibitors
“statins”
• Bile acid sequestrants
• Fibrates
• Phenothiazines
• Tricyclics
• Beta blockers
• Oral contraceptives
• Alpha blockers
(clonidine/methyldopa)
• Butyrophenones (haldol)
• Sulfonylureas (glipizide,
glyburide, tolazemide)
• Biguanides (metformin)
• Bisphosphonates
• Thiazide duiretics
Curcumin
• From turmeric (Curcuma longa) root/rhizome
• One of top selling botanicals globally
• Curcuminoids reported:
• Antiinflammatory
• Decreases inflammasome signaling
• Supports musculoskeletal system
• Joints/connective tissue support
• Helps improve flexibility and mobility
• Antiviral/antibacterial – COVID potential
Curcumin - Metaflammation
• Decreases oxidative stress via Nrf2-keap1 pathway
• Inhibits nuclear factor-kappaB
• Inhibits Toll-like receptor 4-dependent signaling pathways
• Inhibits activation of a peroxisome proliferator-activated receptorgamma
pathway
• Modulates multiple cell signaling molecules
• TNF-alpha
• IL 1, IL-6
• COX-2 and 5-lipoxygenase
• NF-kappaB
• CRP
• PgE2
• TGF-beta
• AST/ALT
• Malondialdehyde MDA
• Lab study reports curcumin ameliorates pancreatic beta cell destruction in
autoimmune diabetes
Issues with Curcumin Bioavailability
• Studies report curcumin (curcuminoids) have poor oral bioavailability
• Poor oral and/or GUT absorption
• Hepatic First pass effect
• Manufacturers have tried to compensate
• Bioperine – Piper sp. (pepper)
• Liposomes
• Now nanotized
• SMART turmeric oromucosal spray
• Superior formulation characteristics:
• SMART COATING – hydro layer
• Particles have positive charge
• 45-50 mV
• cross oromucosal membrane readily
• Particle size to cross membranes effectively
• < 400 nm (0.4 microns)
• STABILITY
• Fformulation tested to be stable for 24 months at room temp
SMART Oromucosal Curcumin Spray Dosage
• 9-18 sprays daily (3-6 sprays TID) = 25mg/ml
• Intensive therapy use higher dosages
• 30ml BPA free plastic
• Nanocurcumin effective at 9% of general oral dose
• Physical stability studies x 24mo – microbial x 16 mo
• Pharmaceutically manufactured - sterile
C3 Reduct Curcumin
• Tetrahydrocurcuminoids (THC) – hydrogenated curcuminoids
• More bioavailable than regular curcuminoids
• Improved anti-inflammatory activity
• Made as LPT oral liposomal tablet
• 25mg THC per LPT in a 350mg proprietary anti-inflammatory base
• Chew/swallow 1 BID
D-Ribose
• Simple sugar
• Replenishes ATP and Recycles Lactic Acid
• Helps normalize heart rate
• Reduces oxidative damage
• Improve Lactate disposal – helps w/ pH
• Improves stamina and endurance
• Rate limiting step for resynthesis of ATP
• Improves ATP production and recovery – improved energy
• Improves glutathione – reduces oxidative stress
• Helps with management of heart rate under hypoxic (anaerobic) load
• Dose = 5-20gm daily
Dihexa
20mg/ml(topical)
(HGF activity enhancer)- reverses the effects of
neurodegenerative diseases, neurocognitive/antidementia properties
Epigallocatechin-3-gallate (EGCG)
EGCG Mechanisms
• Epigallocatechin-3-gallate from Green tea leaves (Camellia sinensis)
• Antioxidant
• Neuroprotective
• Decreases microglial inflammation
• Improves adult neurogenesis in the hippocampus
• Immune supportive
• Decreases proinflammatory cytokine release
• Decreases inflammation
• Antiviral
• EGCG binds to viral cell membrane
• Represses the replication and transcription of virus
• Intake of EGCG is reported inversely associated with the risk of
cardiovascular diseases
• Anxiolytic
• Interaction with γ-aminobutyric acid (GABAA) receptors
• EGCG may inhibit spontaneous excitatory synaptic transmission
independently of GABA receptor activation
• Protects body from heavy metal-induced oxidative stress
• 50-200mg BID
• 21mg LPT – oral liposomal tab, 95% EGCG – chew/swallow 1 LPT BID
• Addition of theanine (200mg w/ each dose of EGCG) can decrease any
negative effects of high dose EGCG
Fermented Wheat Germ Extract (FWGE)
• Source of 2-methoxy-p-benzoquinone (2-MBQ) and 2,6- dimethoxy-p-benzoquinone
(2,6-DMBQ)
• Supports healthy cell metabolism
• Supports aging process
• Enhances Quality of Life
• Cancer therapy – antimetastatic, helps in cachexia
• Immune support
• Promotes NK cells and response of macrophages, B-cells and T-cells
• Improve Th1/Th2 balance
• Dosage
• 2 capsules daily ( 2 caps = 41 mg FWG)
• If over 90 kg (or 199 lbs), use 4 capsules daily
• Take 1 hour before or after meals or other supplements
• Do not use if on immunosuppressive meds
FGL (Fibroblast Growth Loop Peptide)
• Neural Cell Adhesion Molecule (NCAM) mimetic
• Binds to the Fibroblast Growth Factor Receptor 1 (FGFR‐
1)
• Antiinflammatory/antioxidant/neuroinflammation
• Neurological supportive/ Enhanced cognition
• Nasal Spray – 100‐200 mg daily
Fisetin
• 3,3′,4′,7-tetrahydroxyflavone
• first record of fisetin as an isolate from Venetian sumac (Rhus cotinus L.) dates back to 1833
• Flavonoid found in fruits/veggies, i.e. strawberry (highest content), apple, persimmon,
grape, onion, and cucumber
• Senolytic
• Reported to induce apoptosis in aged human umbilical-vein endothelial cells
• Mechanism of senescent-cell apoptosis related to its blocking on the PI3K/AKT
pathway
• mTOR blocked, autophagy activated
• Anti-inflammatory/antioxidant
• Increases glutathione synthesis
• Reported to decrease risk of CHD and CVDs
• 100 mg daily
• Poorly orally absorbed – take w/ fat (ie fish oil) to increase absorption or use
liposomal
GLP-1 agonists
GLP-1 agonist not rapidly degraded by Dipeptidyl peptidase-4 (DPP-4)
Alleviate endoplasmic reticulum stress, regulate autophagy, promote
metabolic reprogramming, stimulate anti-inflammatory signaling, alter gene
expression, and influence neuroprotective pathways
Reduce gastric emptying, increase in satiety and inhibition of food motivated
behavior, replenishment of insulin stores, as well as cytoprotective and antiinflammatory
actions on β-cells
Alleviate glucotoxicity, lipotoxicity, excess nitric oxide (NO), Ca2+ depletion,
oxidative stress, and cytokine-induced ER stress
Facilitate autophagy under chronic exposure to excess nutrients, whereby it
prevents autophagosomal-lysosomal fusion impairment
Improve cardiac function, restore lung function and reduce mortality in patients
with obstructive lung disease, influence blood pressure and lipid storage, and even
prevent synaptic loss and neurodegeneration
GLP-1 based therapies are beneficial to kidney function through increases in renal
blood flow (RBF), urinary flow rate, prevention of rises in plasma creatinine, reduced
tubular necrosis, an increase in renal interstitial fluids and glomerular filtration rate
(GFR), as well as cytoprotective and anti-inflammatory actions through interactions
with the nervous system and the renin angiotensin system (RAS) (Rowlands, 2018)
Re: weight loss, administration of GLP-1R agonists induced BAT thermogenesis
through increased uncoupling protein 1 (UCP1), mitochondrial respiratory chain
element and PGC1α, independent of nutrient intake. Also activate Adiposeresident
invariant natural killer T (iNK) critical to weight loss
START LOW GO SLOW
Liraglutide start 0.6mg SC daily, increase every 3-4 days as tolerated to max 3mg
Semaglutide start 0.25mg SC weekly, increase every 1-2 weeks as tolerated to max
3.4mg
Dulaglutide start 0.75mg SC weekly, increase every 1-2 weeks as tolerated to max 4.5mg
Contraindication: personal history thyroid cancer
SE: NAUSEA, constipation, fatigue, insomnia, weight loss, rare pancreatitis
Dose away from GHS as it enhances somatostatin
• GLP-1 receptor agonists appear to have a favorable safety profile
• NOT FOR USE IN PREGNANCY – discontinue med at least 2 months
before a planned pregnancy
• Most common SE = GI symptoms, mainly nausea; headache
• Injection site reactions – redness, swelling, pruritus
• Severe SE’s include – pancreatitis, allergic reactions, thyroid C-cell
carcinoma
• Several cases report acute kidney injury, primarily through
hemodynamic derangement due to nausea, vomiting, and diarrhea
Glucosamine
• Commonly combined with chondroitin sulfate
• Active Forms: Glucosamine SO4 & HCl
• flexibility; inflammation
• “Trials of glucosamine and chondroitin preparations for OA symptoms demonstrate
moderate to large effects…”
• Chondrocytes use glucosamine as raw material to synthesize proteins that bind water in cartilage: proteoglycans and glycosaminoglycans (GAGs)
• Glucosamine production of hyaluronic acid, which provides shock absorbing &
lubricating properties of synovial fluid
• Dosage: 1500mg/day over 200 lb, = 2000mg/day
• Combine w/ chondroitin for synergistic effects
Green Tea polyphenols
• From Camellia sinensis leaf
• Antioxidant polyphenol
Epigalocatechin gallate (EGCG)
• Antiinflammatory
• Inhibits lipid peroxidation
• Suppresses COX-2, MMPs, TNFalpha, IL-6, 8, 12
• Enhances DNA and cellular repair
• Green tea extract: 500mg daily in divided doses ; std 50% EGCG
• EGCG Lipotab = 21mg 95% EGCG – chew/swallow 1 QD
• High doses of standardized green tea extracts have been reported to cause
hepatotoxicity
• From EGCG > 800mg daily
• Taking EGCG w/ theanine reported to decrease the negative effects
GWO742
• PPAR β/δ agonist
• GW0742 uses:
– Promote muscle regeneration
– Increases exercise endurance
– Supports weight management
– Decreases risk of heart disease – improves BP,
endothelial function
– Accelerates wound healing
– Neurological supportive ‐ cognition
– Supports IR and T2D issues
– Pulmonary issues
– Supports improved eye health
• Lab animal studies report GW0742 improves
metabolic abnormalities
– Including IR in skeletal muscle in mice fed high‐fructose corn syrup
– Insulinotropic activity
• Study results: GW0742 improves glucose
homeostasis in diabetic rats through
activation of PPAR‐δ
GLP1 agonists

Honokiol
• From Magnolia (Magnolia officinalis) bark extract
• Std. to 98% honokiol - pleiotropic lignan
• Honokiol - GABAA binding
• Decreases sleep latency to NREM sleep
• Increases N-REM sleep
• NMDA antagonist
• Anti-inflammatory – decreases NFkB expression; decreases microglial activation
• Readily crosses BBB
• Decreases LPS induced memory deficit
• GABAA binding
• Reduces anxiousness
• Pain modulation
• Endocannabinoid binding
KCF‐18
– Antioxidant/anti‐inflammatory
– Derived from cytokine receptors
– Binds to TNF‐alpha, IL‐1beta and IL‐6 receptors
– Cell experiments demonstrated that KCF18:;;;
• Significantly reduces the binding of proinflammatory cytokines to their cognate receptors
• Inhibited the mRNA and protein expressions of TNF‐α, IL‐1β, and IL‐6
• Reduce the expression of reactive oxygen species induced by
cytokines in human monocytes
• Decreases p65 nucleus translocation induced by cytokines
• Reduces expression of IL‐6 and increased white blood cells
stimulated by lipopolysaccharides
KPV
● A naturally occurring tripeptide: Lysine-proline-valine
● A C-terminal peptide fragment of α-melanocyte stimulating hormone (α-
MSH)
● A small molecule with broad anti-inflammatory effect & antimicrobial action
● In the absence of pro-inflammatory stimuli, LPS/IL-1, there is little to no
immunosuppressive potential of alpha MSH
● Contributes to innate defense; stabilizes mast cells
● No stimulation of melanocytes
L-arginine
○ Amino Acid
○ Improves nitric oxide levels
○ Precursor to creatine
○ Stimulate hGH by suppressing endogenous somatostatin secretion
• Cardiovascular benefits
• Erectile dysfunction
• Safe at moderate doses up to 10 gm
• Normal dose = 2-10gm sustained release daily
• Arginine reported to improve growth hormone AT REST by 100%
L-Glutamine
Glutamine as an anti-fatigue amino acid in sports nutrition. Nutrients. 2019;11(4):863.
Most abundant amino acid (AA) for protein synthesis
Makes up 50% of all AAs in blood and 60% AA’s in tissue
Supports GH levels
Helps maintain muscle mass
Dose = 5-10 gm daily
L-glutamine and GUT
• Protects GI mucosal barrier
• Skeletal muscle contains 60% of body glutamine
• FUEL
• Involved in glutathione synthesis
• Protects against endotoxemia
• Substrate for Growth hormone release
• Supports microfloral health
• Helps maintain secretory IgA
• Prevents attachment of bacteria (i.e. H pylori) to mucosal cells
• Inhibits gram-negative translocation of bacteria from colon
• Major fuel for enterocytes and colonocytes
• Maintain integrity and function of mucosal barrier
• Improves height of villi
• Reduces villi permeability
• Reduces leaky gut syndrome symptoms
• Defends against food allergies and intolerances
• Protects against injury and inflammation including drug induced (NSAID
damage)
• Helps in chemotherapy induced GUT damage
• Supports IBD - Crohn’s and UC
• Helps in ulcers – decreases mucosal apoptosis
L-Theanine
• Amino acid found in green tea (Camellia sinensis)
• Acts antagonistically against the stimulatory effects of caffeine in the tea on the
nervous system
• Glutamate antagonist
• Indirectly increases GABA (gamma-amino-butyric acid)
• balances the excitability that can sometimes lead to restlessness, insomnia,
and other disruptive conditions
• Antianxiety
• Cognitive and mood support
• Increases levels of dopamine
• Dampens Phenylethylamine (PEA)
• Increases alpha waves
• Good for sleep if daytime drowsiness a problem
• 200-400mg up to 4 times a day
Larazotide (oral)
- restores intestinal barrier, tight junction regulator, enterocyte
proliferation, suppresses pro inflammatory signaling pathways, protection against
apoptosis and cellular stress ( FDA fast track designation for celiac disease )
Macimorelin
• Growth hormone secretagogue (GHSR) agonist
• Stimulates GH release
• Binding potency to the GHS‐receptor in animal and human
tissues similar to that of ghrelin and peptidyl GHS
• Used for:
– Growth hormone support
– Performance support
– Improved body composition – weight management
support
Garcia JM, et al. J Clin Endocrinol Metab. 2013;98(6):2422‐29
• GHRYVELIN (Aeterna Zentaris, EU)
• MACRILEN (US)
• Both indicated for GH insufficiency
• Dosage of MACRILEN and GHRYVELIN to Dx GH
deficiency
– Oral granules
– 0.5mg/kg x 1
• Transient Side effects include:
– Metallic taste
– Fatigue
– Headache
– Nausea
– Dizziness
– Diarrhea
– Acute Hyperthermia – feeling “hot”
• Potential Drug Intx
– Avoid drugs that prolong QT interval
Antipsychotics – chlorpromazine, haloperidol, thioridazine,
ziprasidone
Class 1A antiarrhythmics – quinidine, procainamide
Antibiotics – moxifloxacin
Class III antiarrhytmic meds – amiodarone, sotalol
– Discontinue CYP34A inducers
St. John’s wort
Modafinil
Others Garcia JM, et al. J Clin Endocrinol Metab. 2013;98(6):2422‐29
Magnesium
Magnesium bisglycinate chelate
• Co-factor in over 300 biochemical reactions
• Over 75% of Americans are Magnesium deficient
• Help support sleep quality and quantity
• Helps improve restless leg syndrome, cramps and muscle spasms
• Mg in Sleep – improves GABA levels
• Magnesium critical in over 400 biological reactions
• 70% Americans deficient in magnesium
• Many drugs deplete magnesium – diuretics, PPIs, HRT/OCs, others
• Obesity depletes
• Magnesium supplementation:
• Improves GLUT4 in skeletal muscle
• Improves glycogen synthesis
• Improves pancreatic beta-cell proliferation and regeneration
• 400-800mg elemental magnesium per day, as chelate .
• Magnesium supplementation 500mg elemental form for 4 wk in overweight
individuals: distinct changes in gene expression
• C-peptide .4ng/ml
• Insulin -2.2uU/ml
• 24 gene up regulation and 36 down regulation
• All related to metabolic and inflammatory pathways
Magnolia/ Phellodendron
• Proprietary blend of Traditional Chinese Herbs Magnolia officinalis and Phellodendron
amurense barks
• Marketed for stress-related appetite control and reduction of stress-related fat
deposition
• Contained in multiple company formulations
• Anti-anxiety and anti-stress properties rival benzodiazepines, yet non-sedating
• Helps normalize cortisol and DHEA levels, including exercise induced
• Helps decrease food cravings associated with increased stress
• Low side-effect profile
• 250mg 2-3 times a day
Melatonin
• Natural sleep hormone
• The circadian counter-hormone to Cortisol
• Decreases with stress, hormonal imbalances
• Improves circadian insulin production
• Used for sleep problems
• Antioxidant
• Convincing evidence for exogenous melatonin in:
• Reducing sleep onset latency in primary insomnia
• Delayed sleep phase syndrome
• Regulating the sleep-wake patterns
• Authors conclude melatonin is of great value in treating certain first-degree sleep
disorders
Auld F, et al. Evidence for the efficacy. Of melatonin in the treatment of primary adult sleep disorders. Sleep
Med Rev. 2017;34:10-22.
Melatonin DIND – Drug-Induced Nutrient
Depletion
Melatonin is reported to be depleted by:
• Beta-blockers
• Calcium channel blockers
• Benzodiazepines
• Estrogen-containing medications
• Hydralazine
• Loop diuretics
• Theophylline
• Antidepressants, including SSRI (Selective serotonin reuptake
inhibitors)
• NSAIDs (Non-steroidal anti-inflammatory drugs)
Met‐Enkephalin
• Methionine Enkephalin AKA opioid growth factor, FK
33‐824
• Opioid neuropentapeptide
• Potent delta‐opioid receptor agonist
– Much less for μ‐opioid; None Kappa
• Produces anticonvulsant, anxiolytic, analgesic and
antidepressant like effects
Jankovic BD. Enkephalins and immune inflammatory reactions. Acta Neurol
(Napoli). 1991;13(5):433‐41.
• Involved in humoral and cell‐mediated immune reactions
• Immunomodulatory – increases IL‐2, T cells, NK cells
• Lower doses stimulate PMNs, higher depress immunity
• Anti‐inflammatory
• Human studies have used:
– IM dose 0.2‐0.5mg
– SQ –10‐80mcg/kg 3 x weekly
– IV infusion 250mcg/kg over 30 min
MK-677 (oral)
orally active GH secretagogue, reverses diet induced catabolism, post
injury and surgery tendon, ligament, muscle injuries
Nicotinamide Riboside (NR)
• Supports neuronal NAD+ synthesis
without inhibiting sirtuins
• Sirtulins - important regulators of metabolism and longevity
• NAD+ is a rate-limiting co-substrate for sirtuins enzymes
• NR regulates sirtuins function and subsequent regulation of oxidative metabolism
• Activation of NAD+ expression linked with a decrease in beta-amyloid (Aβ) toxicity in
Alzheimer's
• PGC-1α - a crucial regulator of Aβ generation
• Affects β-secretase (BACE1) degradation
• Helps promote peroxisome proliferator-activated receptor-γ coactivator 1 (PGC-1α)-
mediated BACE1 ubiquitination and degradation
• Orally available commercial product containing nicotinamide riboside is patented
• Oral Dose 250-500mg daily
• May also be used intranasally and/or sublingually in combination with Rg3 and
methylcobalamin
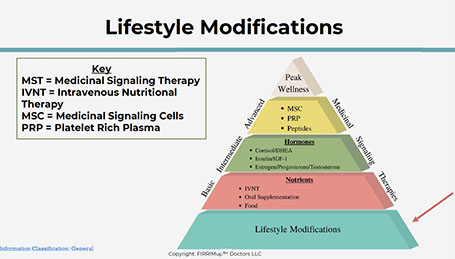
Phosphotidic Acid (PA)
Why Supplement With Phosphotidic Acid
(PA)
• Normally, small amount of PA present in muscle matrix
• PA is biosynthesized from phospholipids to small degree on an ongoing basis
• Mainly for cell membrane use
• Intrinsic amount of PA is just sufficient to impact mTOR signaling
• at a base level, even during exercise,
• Thus MPS and muscle accretion are continually compromised.
• Orally ingested PA provides an optimal amount of PA
• Critical requirement for sig. driving mTOR signaling
• Hence driving MPS and muscular hypertrophy
PA’s Effects On mTOR & MPB
• After an oral dose of PA and during mTOR signaling, MPB is reduced, thus
preserving existing muscle mass.
• PA is considered effective “anti-catabolic” nutrient.
• PA plays a role in “Anabolic Resistance”: Impaired rate of cellular anabolism in
response to various anabolic stimuli.
• Anabolic Resistance is the impaired ability to build muscle caused by an excess
calorie consumption over time.
• PA supports minimizing age related muscle loss (sarcopenia*)
• Dose 750mg-1500mg per day
• * Age-related loss of muscle protein is attributed to imbalance between MPS and
MPB rates, resulting in a negative muscle protein balance and, over time, a decline
in skeletal muscle mass.
Phosphatidylcholine
• Promotes cognitive function
• Improves neurological health
• Increases SIRT-1 expression
• Helps decrease vascular cognitive impairment
• A 2005 Cochrane Database Systematic Review reported evidence supporting use
of proprietary phos-choline in vascular dementia
• 250-500mg BID
Phosphatidylserine
• Phospholipid found in cell membranes
• Antioxidant
• Associated with improving brain and neurological function
• Also reported to help balance testosterone to cortisol ratio in response to
stressors
Plant Sterols/ Sterolins
• Improved cortisol/DHEA ratio
• Improved Th1/Th2 balance
• Supportive in Autoimmune Thyroiditis
• Adults: 1-2 capsules three times daily on an empty stomach – can
bind to cholesterol/lipids
• > 200 lb = 2 caps TID
• Children: one capsule twice daily (5-12yrs)
• 12 yrs and older can take adult dosage
• New Extra strength version – 30mg sterols/0.3mg sterolins per cap;
1 cap BID
Probiotics
• Probiotic flora consists of over 400
species of bacteria
• Enhanced immunity
• Interact with mucosal cells of GUT to provide a barrier against pathogens
• Microfloral imbalances
• Overtraining; intense physical exercise
• Poor food choices – high sugar, pesticides, additives, preservatives, antibiotics,
hormones, red meats
• Chronic stress
• Impure water
• Drugs
• 15-20 billion CFU QD
• Special 12 species probiotic – 60 billion CFU 1 cap daily
• Synthesize short chain fatty acids (SCFA)
• SCFA a primary source of fuel for intestinal epithelial cells, keeps them from flattening out.
• Butyrate - helps remove lipid soluble toxins
• Butyrate protects intestinal cells from abnormal growth, and may protect against colon cancer
• SCFA’s improve acidic environment in the intestines
• Acidic environment decreases pathogenic overgrowth
• Meta- analysis 1970-2011
• 79 randomized, controlled trials in 10,351 patients comparing probiotic to placebo
• 11 probiotic strains
• The Question - Are probiotics beneficial in treating gastrointestinal diseases, including
• Infectious diarrhea
• IBS
• H. pylori infections
• C. Difficile
• Antibiotic Associated Diarrhea
• Traveler’s Diarrhea
• Necrotizing entereocolitis
• Pouchitis
• The results: YES for all (statistically significant positive outcomes over placebo)
Pyrroloquinoline quinone (PQQ)
• Antioxidant
• Influences energy-related metabolism and neurologic function
• Reported to stimulate biogenesis of mitochondria
• Helps decrease inflammatory pathways (IL-6, CRP)
• Dose = 15-45mg daily
Rg3 Ginsenoside
• Ginsenosides are bio-active saponins found in ginseng (Panax ginseng,C.A.
Meyer) root
• About 150 ginseng saponins are known
• > 90% are classified as Rb1, Rb2, Rc, Rd, Re, Rg1, and Rg3
• Rg3 ginsenoside is formed after steaming the roots of Panax ginseng
• Rg3 makes up approx. 0.1% of total ginsenoside
Rg3 Physiological Properties (lab and human studies):
• Antioxidant
• Antiinflammatory
• Neuroprotective
• Antiaging
• Anticancer
• Metabolic syndrome support
• Vascular protective
Rg3 Neuro-Pharmacology
• Neuroprotective
• Decreases oxidative stress-induced inflammation
• Improves neuroinflammatory outcomes
• Helps attenuate microglial activation
• Decreases neuroinflammation
• COX-2 inhibition
• Inhibition of matrix metalloproteinase-9 (MMP-9)
• Improves NO and ROS (reactive oxygen species) levels
• Decreased inflammatory mediators - TNF-alpha, IL-1Beta
• Antinociceptive in lab animals – decreases pain
• Decreases excitotoxicity
• Attenuates NMDA (glutamate) receptor-mediated currents
• Decreases NMDA-induced neurotoxicity
• Inhibits L-type Ca(2+) channels
• Counters increased levels seen in microglial activation
• Dosage Intranasal:
• Intranasally added to Methylcobalamin + Nicotinamide riboside
• 2 sprays in each nostril 2 times daily
• Standardized to 90% (R) Rg3
• Used to support improved mitochondrial health and cognitive function
• LPT = proprietary oral liposomal tablets
• Rg3 LPT uses purified 85-90% Rg3 "R" ginsenoside
• LPT designed for average particle distribution of 100 nm
• Patent-pending liposome platform
• Improved absorption, improved bioavailability
• Rg3 LPT is highly advanced technology in a convenient, solid, chewable dosage
form
• 15mg LPT, ½ - 1 QD chewable
Selank
6mg (intranasal)
(Cell signaling- anxiolytic)- antidepressant, decreases anxiety,
positively influences memory and learning process, enhances GABA
Semaglutide sq- (GLP-1 agonist)
decreases appetite, slows gastric emptying, reduces
percent body fat, cardioprotective, improves cognitive function, antiinflammatory, lowers
HgA1c levels
Sermorelin (GHRH)
GHRH analog derived from the first 29 amino acids of the GHRH protein
Sermorelin also produced small acute rises in prolactin, FSH, and LH like endogenous GHRH and increased testosterone
10 elderly men treated either 0.5 mg or 1 mg bid for 14 days on and 14 days off
Sermorelin treatment resulted in elevations in IGF-1 in a dose-response fashion to levels approaching those of the younger men
Elevations in IGF-1 remained above baseline levels in the elderly men even 2 weeks after stopping sermorelin
-improved sleep quality, increase in cognitive function, quicker
recovery times post-injury, increase in muscle mass, increase in strength
increase in IGF-1 levels, improved sleep quality, increase in
cognitive function, quicker recovery times post-injury, increased muscle mass, increase in
strength
SS‐31
• Aka elamipretide, Bendavia
• Mitochondrial peptide
• Uses:
Antioxidant/antiinflammatory
Mitochondrial protection/ stabilizes cardiolipin
Anti‐aging
Neurological protection / cognitive/memory support
Alzheimer’s Disease support
Brain injury support
Musculoskeletal injury support
Cardiomyopathy support
Kidney support
Ophthalmic – atrophy in dry Aged‐related macular
degeneration support (AMD)
• Preclinical studies suggest benefits in muscle aging, atherosclerosis,
ischemia, osteoarthritis, diabetes, and glaucoma.
Types of evidence:
1 phase 3 double‐blind randomized controlled trial in primary mitochondrial
myopathy
1 phase 2/3 randomized controlled trial in Barth syndrome patients
1 double‐blind phase 2 RCT in patients with heart failure
1 double‐blind phase 2 RCT in patients with primary mitochondrial myopathy
1 double‐blind phase 1/2 RCT in patients with primary mitochondrial
myopathy
1 double‐blind phase 2a RCT in patients with myocardial infarction
2 double‐blind randomized controlled trials, 1 in patients with
atherosclerotic renal artery stenosis and 1 in heart failure
1 pilot clinical study in renovascular hypertensive patients undergoing renal
revascularization
Numerous preclinical studies
Birk AV, et al. J Am Soc Nephrol. 2013;24(8):1250‐61.
Dosage:
SubQ
• 40 mg SubQ daily x 12‐24 weeks
Oral
• 10‐50 mg daily
TB4 frag (oral)
–(multi- functional regenerative peptide). – thymus extract
Tesamorelin
Stabilized analog of human GHRH
FDA approved for HIV lipodystrophy
Wang, Y. “Tesamorelin, a Human Growth Hormone Releasing Factor Analogue.” Expert
Opinion on Investigational Drugs 18, no. 3 (March 1, 2009): 303–10.
2 strong studies in mild cognitive impairment demonstrating appropriate
increases in IGF-1 and improved neurotransmitter formation and cognition
Thai Ginseng (Kaempferia parviflora) root
• Aka Black ginger – used in SE Asia as a food and medicine
• Contains high level of antioxidant polymethoxyflavones
• Specifically 5,7 dimethoxyflavone
• Improves mitochondrial biogenesis – increased energy
• SIRT-1 upregulation - 3-4x that of resveratrol
• Sirtuins involved in metaflammation
• Sirtuins are also evolutionarily viral restriction factors - antiviral
• 100-200mg AM daily std. to 4-5% 5,7 dimethoxyflavone
• Although Thai ginseng is a WEAK PDE5 inhibitor, use with caution if patient taking
prescribed PDE5 inhibitors
Thymagen
• AKA Thymogen, Vilon®
• Dipeptide bioregulator
• Glu‐Trp (L‐glutamine/L‐tryptophan)
• Primary effects on thymus – immune support
• Originally isolated from calf thymus (natural thymic factors ‐ larger peptide called Thymalin)
– Now bioregulators are produced synthetically
thru DNA recombinant technology (Thymagen, Thymogen)
• As a bioregulator, supports Th1/Th2 balance
• Induces differentiation of T cells
• Enhances T cell function
• Prevents overproduction of inflammatory cytokines – cytokine storm
• Anti‐inflammatory/analgesic activity
– Acts directly on afferent nerve terminals through
prostaglandin‐E2 (PGE2)‐dependent mechanisms
• Activates neutrophil chemotaxis and phagocytosis
• Applications for Thymagen include:
– Chronic inflammatory conditions
– Tissue repair disorders
– Stress‐induced immuno‐depression
– Optimization of cancer immuno‐therapy,
chemotherapy and radiotherapy
– Age‐related immune dysfunction
Dose:
• General dosage = 100‐200mcg SubQ every 3 days x
15 days
• Therapeutic or preventative
• Repeat at least twice annually for prevention
• Synergistic w/ conventional Rx therapy ‐ no interactions
Thymosins: TA1/Tβ4
● Thymosins: discovered in the mid 1960’s
when Dr. Goldstein from Albert Einstein
College of Medicine (NY) studied the role of
the thymus in the immune system
● 2017: TA1 & TB4 → Topics include:
○ Immunomodulation, ID, Sepsis, Liver
dx, Eye dx,
○ Neuro --- CVA, Alz Dx, severe TBI,
○ Cardiac---vascular and stem cell effects
Thymosins: TA1
Thymosin is a “hormone” (smart small molecule) secreted from the thymus. Its
primary function is to stimulate the production of T cells, which are an important
part of the immune system. Thymosin also assists in the development of B cells
to plasma cells to produce antibodies.
Thymosin α1 (Tα1) is an immunostimulatory peptide that is commonly used as
an immune enhancer in viral infectious diseases such as hepatitis B, hepatitis C,
and acquired immune deficiency syndrome (AIDS).
Thymosin alpha 1 is usually administered twice a week via a subcutaneous
route. The standard single dosage ranges from 0.8 to 6.4 mg, while multiple
doses range from 1.6 to 16 mg for five to seven days.
When prescribed by a licensed healthcare provider for a legitimate medical purpose,
using FDA-approved peptides is generally considered legal. However, off-label use or
self-administration of peptides without proper medical supervision can result in legal
consequences and potential health risks
Thymosin Beta 4
● Regulates the cell/muscle building protein
actin
● Displays potent anti-inflammatory effects
● Promotes wound healing and angiogenesis
● Clinical trials have demonstrated its ability
to reactivate progenitor cells to repair
damaged tissue
● Due to its LMW, TB4 is able to
‘hone’; it has the ability ‘to
travel’ to the site of injury.
● Prevents adhesion and fibrous
band formation in injured
tissue– i.e. muscles, tendons,
and ligaments
● Protects and restores neurons
post TBI
● Promotes rapid wound healing with little-to-no
scarring
● Supports tissue stem cell vitality and
proliferation to regenerate and heal injured
tissue
● Promotes angiogenesis and actively combats
sarcopenia
● Anti-inflammatory properties help reduce
chronic and acute pain
Dosing:
● TB4-frag 150 mcg po per capsule
● TB4-frag plus 150 mcg po per capsule + Natural thymic
extract 350 mcg
TP508
• Non‐proteolytic thrombin peptide
• AKA rusalatide acetate, Chrysalin®
• Used for:
– Vascular damage including myocardial ischemiac
– Musculoskeletal injuries
– Wound healing®
– Chronic inflammatory issues including:
oSARS‐Cov2 infection
oAcute lung injury ‐ Acute Respiratory Distress
Syndrome (ARDS)
oChronic smoke inhalation
oMusculoskeletal injuries
oRadiation damage – radioprotective, including GUT
crypt cells
Ryaby JT, et al. J Bone Joint Surg Am. 2006;88(suppl 3):132‐139
• TP508 reported to initiate tissue repair and
regeneration by:
– Reversing endothelial dysfunction
– Stimulating revascularization
– Attenuating inflammation
– Stimulating NO production
– Reducing apoptosis
• Protects crypt cells in the GUT exposed to radiation
• Significantly increases expression of both LGR5 and
DCLK1 stem cell markers in intestinal crypts
• Also increases number of DCLK1‐positive cells per
crypt
Kantara C, et al. Lab Invest. 2015;95:1222‐33.
oSubQ – Locally for injury/wound
For injury healing – 10 ‐ 30 mcg SubQ at site of injury x1 single dose
Must be given w/in 24 hrs of injury
•
oSubQ – for aesthetics
15 units to site
Give 4 times, 1 month apart then repeat annually
•
oTopically
10 mcg TP508 in small amount saline, apply to area then cover wound
with foam bandage
Use this twice weekly along with routine wound care.
Ryaby JT, et al. J Bone Joint Surg Am. 2006;88(suppl 3):132‐139
Type II Collagen
• Novel, undenatured type II collagen
• Derived from chicken sternum cartilage
• Basis of articular and hyaline cartilage
• Increases synovial fluid production from the synovicites
• Small doses of collagen inhibit T-cell attack
• Collagen accumulation reduced after major surgery
• Pre-surgery radiation cancer patients significantly inhibits collagen
accumulation
• Corticosteroids/NSAIDs reduce collagen synthesis also
• Clinical studies report benefits from collagen use in RA and OA and in wound
healing post surgery
• 40 mg daily (20mg BID)
Vasoactive Intestinal Peptide (VIP)
• The twenty-eight amino acid peptide is structurally related to the
secretin/glucagon family of peptide hormones, sharing 70% sequence
identity with the neuropeptide pituitary adenylate cyclase-activating
polypeptide
• VIP is produced by neurons, endocrine and immune cells, and is
present in most organs including the CNS, heart, lung, thyroid, kidney,
urinary and gastrointestinal tracts, genital organs and the immune
system.
• Regulates Circadian rhythms
• Noncholinergic relaxation of vascular and nonvascular smooth muscle
• Increases neuronal survival and regulates glycogen metabolism in the
cerebral cortex
• Promotion of embryonic growth and brain development
• has neurotrophic effects and regulates bone metabolism
• Increases insulin and glucagon secretion
• Increases blood flow in thyroid but has no effect on hormone levels
• Promotes the release of prolactin, luteinizing hormone, and growth
hormone from the pituitary gland, and regulates insulin and glucagon
release
Regulates cardiac contractility
• Coronary and systemic vasodilatation
• Increases glycogenolysis and lowers arterial blood pressure
• Increases cardiac output
• Relaxes airway and pulmonary vascular smooth muscle
• Inhibits airway and pulmonary vascular smooth muscle proliferation
• Bronchodilatation
• Macrophage- deactivating factor
• Regulates the differentiation of CD4+ t cells
• Anti-Inflammatory
• Defense mechanism against septic shock
• Increases the secretion and inhibits the absorption of intestinal
luminal fluid
• Relaxes smooth muscle and mediates distension-induced reflexes
• Decreases intestinal paracellular permeability
• Increases epithelial cell proliferation
• Releases pancreatic enzymes
• Nasal Spray
• Lipotabs 100mg
Patients with autoimmune diseases such as lupus, autoimmune thyroiditis, MS and RA have low levels of VIP in serum, associated in some cases with high levels of VIPase autoantibodies
VIP reduces the clinical and histopathological severity of mouse model crohn’s disease (CD) and reduces weight loss, diarrhea, and macroscopic and microscopic intestinal inflammation
reduced the levels of various chemokines and pro-inflammatory cytokines, such as tumor necrosis factor-α (TNF-α), IL-6, IL-12, and IL-10
In patients with food allergy, VIP stabilizes the expression of IL-10, Bregs, and restores immune regulation function, thereby reducing the food allergy response
VIP-/- mice demonstrate reduced proliferation and migration of intestinal epithelial cells (IEC) and their increased apoptosis, resulted in increased intestinal permeability
regulates the Th1/Th2 balance by directly acting on T cell differentiation and indirectly
regulating the antigen presenting cell function
VIP also inhibits the transcription factors AP-1, nuclear factor-κB (NFκB), CREB, and IRF-1, and impairs the acquisition of the macrophage proinflammatory polarization profile
Systemic administration of VIP causes cardiovascular and gastrointestinal side
effects including a marked decrease in blood pressure, tachycardia,
cutaneous flushing, and watery-diarrhea syndrome
Nebulized VIP in a single 100-microg dose in 20 patients with idiopathic
pulmonary arterial hypertension produced small and temporary but significant
selective pulmonary vasodilation, an improved stroke volume and mixed
venous oxygen saturation. Overall, six patients experienced a pulmonary
vascular resistance reduction of >20%
Check lipase prior to administration
Zinc Carnosine
• Zinc ions bound to L-carnosine
in a 4:1 ratio
• Advanced gastric cytoprotection
• Helps improve integrity of GI mucosa
• Protects against sensitizing proteins, i.e. gluten or casein
• Helps establish lower pH environment in hospitable to H. pylori
• L-carnosine helps transport zinc to heal tissue
• Improves cell migration to wound
• Increases cell proliferation and tissue repair
• Reported to protect against indomethacin-induced gut permeability changes in humans
• 1 cap BID
• Contains/cap:
• Zinc (as zinc carnosine) 17 mg
• Zinc-carnosine (chelated) 75 mg
Zizyphus
• Jujube (Ziziphus jujuba or Ziziphus spinosa) fruit extract 4:1
• Reported to improve sleep quality
• Anxiolytic, sedative and hypnotic effects in laboratory studies
• Neuroprotection
• Increases hippocampal neurogenesis
• Decreases neuro-oxidative stress
• Improves memory and learning
• Synergistic addition to Honokiol for sleep regulation
thymosins


Selective androgen receptor
modulators (SARMs)
IF I am So Fit,
Why is My Testosterone Low?
• Free Testosterone/Cortisol Ratio Important Indicator
• Higher the ratio the better the training gains
• As Cortisol raises and Free and Total Testosterone lowers shifts occur
- More cortisol made from DHEA – less DHEA makes testosterone
- Immune changes tendency toward more allergies (food 7
environment)
-Anabolic drive reduces, gains from training disappear
-Inflammation signaling increases
-Gut breaks down becomes more “Leaky”
- Mood Alters
Cortisol and Sex Hormone Imbalances
• Increased cortisol blocks T4 conversion to T3
• TRH is up-regulated to create more T4
• Increasing TRH will increase prolactin which in turn
• Down regulates LH and FSH production which
• Down regulates testosterone
• As testosterone goes down, so does growth
hormone
Testosterone and the Heart
• In men, T levels begin to decrease after age 40
• Associated with an increase in all-cause mortality and cardiovascular (CV) risk
• Increases risk of developing coronary artery disease (CAD), metabolic syndrome,
and type 2 diabetes
• Reduced T levels in men with congestive heart failure (CHF) results in a poor
prognosis and associated with increased mortality.
• Studies have reported:
• Reduced CV risk with higher endogenous T concentration
• Improvement of known CV risk factors with T therapy
• Reduced mortality in T-deficient men who underwent T replacement therapy
versus untreated men
• Testosterone replacement therapy (TRT) reported to:
• Improve myocardial ischemia in men with CAD
• Improve exercise capacity in patients with CHF
• Improve serum glucose levels, HbA1c, and insulin resistance in men with
diabetes and prediabetes
CONSEQUENCES of Low T in Men
• Frailty
• Reduced lean body mass
• Reduced muscle strength
• Increased total body and
central obesity
• Reduced cognitive function
• Decreased/Low libido
• ED
• Loss of body hair
• Weight gain
• Mood changes
• Increased cardiometabolic
issues – IR, dyslipidemia,
atherosclerosis
• Poor athletic performance
• Increased mortality
Consequences of Low T in Women
• Fatigue
• Muscle weakness
• Increased CV events
• Sleep disturbances
• Reduced libido
• Decreased sexual satisfaction
• Weight gain
• Fertility issues
• Irregular menstrual cycles
• PCOS
• Vaginal dryness
• Loss of bone density
• Poor athletic performance
• Increased mortality
Low Testosterone and Sleep
• Testosterone levels display circadian variationPeak during sleep
• Superimposed on this are burst-like increases in testosterone production
• Occur every 90 min or so
• due to pulsatile LH secretion
• Increase in T during sleep requires at least 3hr sleep
• Sleep disorders can reduce T levels1
• Low total testosterone may affect overall sleep quality
• Especially older men
• Improved by T replacement
• Low T doesn’t seem to affect OSA (sleep apnea)
What are SARMs?
• Steroidal SARM vs. Nonsteroidal SARM
• Nonsteroidal SARMs pioneered by scientists at Ligand Pharmaceuticals and the
University of Tennessee, Knoxville
• Synthetic drugs w/ effects similar to testosterone
• Lignans that bind to cellular androgen receptors - modulate
• Found in some body building and performance enhancing supplements
• Still FDA unapproved for human use
• Used to increase muscle mass, decrease fat, improve bone density, performance
• Non-steroidal anabolic
– More non-specific binding
– Produce undesired effects or pharmacokinetic profiles
• Selective receptor stimulation more desirable than ”conventional” testosterone
support
Uses of SARMs
• Sold as research chemicals – similar to peptides
• Performance enhancing - for “bulking” and “cutting”
• Stacking – combinations of SARMs used
• Studied as potential treatments for
• Male contraception
• Cancer – breast, prostate CA
• Osteoporosis, improved BMD
• BPA – prostate issues
• Sexual dysfunction
• Multiple sclerosis, muscular dystrophy
• Alzheimer’s disease
• Cancer related Cachexia
• Sarcopenia
• Frailty; anti-aging
Why SARMs?
• As men and women age, GONADAL axis becomes imbalanced
• Lose skeletal mass, strength, power
• Mostly due to preferential loss of type 2 muscle fibers
• Increases risk of:
• Falls
• Fractures
• Mobility limitations
• Physical disability
• Poor QOL
• Functional decline and dependence in older individuals place a large burden on
health care services and costs
• Potential to improve skeletal muscle remodeling and gains in skeletal muscle
strength and muscle mass are based on circulating testosterone levels
• Administering anabolic steroids full of adverse effects
• Erythrocytosis
• Leg edema
• Prostate events
Potential SARMs Benefits
• High oral bioavailability
• Similar effects to testosterone (libido, strength gains, fat loss etc.…)
• No conversion to dihydrotestosterone (DHT) by 5 alpha-reductase
• No aromatase conversion to Estrogens
• Improved bioavailability vs. oral steroids/prohormones
• No significant liver toxicity from methylated compounds
• Does not inhibit your HPTA – hypothalamus-pituitary-testicular-adrenal
axis - to the large extent of steroids (no large reduction in LH or FSH)
Available SARMs
• Acadibol (ACP-105, AC-262536)
• Andarine (GTX-007, S4, S-4)
• Ostarine/Enobosarm (MK-2866, GTX-024)
• LGD-3033
• Ligandrol (LGD-4033)
• Stenabolic (SR-9099)
• Testolone (RAD-140)
• S-22
• S-23
• YK-11 (TK-11-OA)
• YK-500
• Cardarine, Endurobol (GW-501516) –
PPAR-omega agonist
• GSK2881078
• Ibutamoren (MK-677) – not for
compounding
Most Popular SARMs*
• Ostarine (MK-2866) - developed in 1990s
• Ligandrol (LGD-4033)
• Testolone (RAD-140)
• Andarine (GTx-007, S-4)
SARM Potential Side Effects
• Phase I and II trials, the first generation ORAL SARMs
have reported:
• Significant reductions in HDL cholesterol
• Significant reduction in SHBG concentrations
• Mild transient elevations of AST and ALT
• Insulin resistance, blood glucose dysregulation
• Headache, nausea, fatigue, back pain
• Altered parameters return to normal after cessation of tx – even at
doses 10x clinical
• Systemic administration may reduce these finding
Other potential SE’s
• Decreased endogenous testosterone
• Reduced sex drive
• Erectile dysfunction
• Infertility issues
• Muscle weakness
• Loss of bone density
• Weight gain accompanied by increased body fat
• Insomnia
• Depression
THE IMPORTANCE OF A PATHWAY TEST
• If the patient is takin estrogen, or birth control
pills, that estrogen can go down CIP1A1
pathway, it’s a very protective pathway and can
help protect from cancer
• If it goes down 16HIDROXY STRONE pathway, is
not that safe it’s a stronger estrogen
• And if it goes down 4HIDROXI STRONE this one
damages DNA its carcinogenic
Drug Interactions studied:
• Ostarine (and its major metabolite) and itraconazole, probenecid,
celecoxib, and rosuvastatin
• No clinically relevant or significant results
• Whether “stacking” SARMs increases side effects or drug interactions
is not known
• 2017 – FDA issues public advisory statement
• “SARMs were being included in bodybuilding products and that these
compounds posed an increased risk for heart attack, stroke, and liver
damage”
• FDA issues warning letters to several distributors for products containing
SARMs
• Products labeled as “dietary supplements” but deemed NOT by FDA
• Potential for life threatening reactions, including liver toxicity
• SARMs also have potential to increase the risk of heart attack and stroke
• Long-term effects on the body are unknown
SARMs - Safety
• Most important point - DO NOT PURCHASE from the INTERNET – Purchase from
Compounding Pharmacies
• 2017 study – compared chemical identity/amounts of ingredients of SARM
dietary supplements and products marketed and sold through the Internet
• Compared the analyzed contents to their product labels
• Study - 44 products marketed and sold as SARMs were tested
• Only 52% contained one or more actual SARMs as labeled
• No actives were detected in 9%
• FINAL RESULTS: Only 41% of internet products were labeled appropriately
SARMS - Cautions
• DO NOT USE INTERNET PRODUCTs
• Dosages and durations need to be followed
• Potential interactions reviewed – drug, food, supplement
• Monitor labs
• T free, total and bioavailable
• DHT
• SHBG
• Estrone
• Estradiol
• Liver enyzymes, bilirubin


Circadian Rhythm and Genes
• Clocks in cells are run by genes, the proteins CLOCK and BMAL1 act as activators,
and members of the periods (PER) and cryptochrome ( CRY) families are repressors
• Receptors in the retina receive light cues, which are carried through the
hypothalamic optic tract and transmitted to the SCN, resulting in its
SYNCHRONIZATION
• Clocks in organs and tissues ( peripheral clocks) can be changed by feeding
rhythms, exercise, social activity, temperature, humidity
Circadian Rhythm and synchrony with nature
• Disharmony and disturbance with
the circadian clock will lead us to
disease
• Lifestyle, shift work at night, sleep
cycle, food habits
• Mutation in circadian genes
• Metabolic obesity, cardiovascular
disease, phycological behavioral
Circadian Desynchrony
• CNS: depression
• Pancreas: Hyperinsulinemia
• Muscle: Insulin resistance,
sarcopenia
• Adrenals: Chronic Fatigue
• Hematopoietic: Autoimmunity
• Vasculature: thromboembolic
events
• Intestine: Dysbiosis
• Adipose: obesity
• Liver: dyslipidemia
Disruption of the circadian Rhythms
• When the circadian rhythms get
broken, dysregulation of the
circadian genes PER,CRY,BMAL1
• Our epigenome starts changing
Sleep
• Most individuals should obtain at least 7-9 hours of quality sleep a night
(Centers for Disease Control, CDC, 2011).
Centers for Disease Control (CDC). www.cdc.gov.
• 67% of Americans experience frequent problems sleeping
• 43% say lack of sleep interferes with their daily activities.
• Between 9-12% of the population are clinically diagnosed with insomnia
Insomnia or disrupted sleep
• Disruption of the circadian rhythm
• Alters Growth Hormone release
• Increases TNF alpha, IL-6
• Increases insulin resistance
• Contributes to weight gain
• Alters Digestive health
Sleep support
Melatonin ( sleep regulator)
• natural hormone supports sleep cycles
• Antioxidant
• decreases w/ age
• Improves circadian insulin production
• Used for sleep problems
• Antioxidant
• 3-20mg 1 hr before bedtime
• Watch for paradoxical effects
Stress Reduction:
1. Glycine has been suggested to have an anxiolytic (anti-anxiety) effect,
potentially reducing stress and promoting a calm state conducive to sleep.
2. By modulating neurotransmitter activity, glycine may help individuals unwind
and relax before bedtime, leading to improved sleep outcomes.
Sleep Disorders:
• Glycine supplementation has shown promise in certain sleep disorders. For
example, studies have explored its potential benefits in individuals with insomnia,
sleep apnea, and restless leg syndrome.
Intermittent fasting
• Stimulates growth hormone Improved cognition
• Decreased neurodegeneration
• Stimulates brain derived neurotrophic factor (BDNF)
• Weight loss
• Improved blood pressure
• Cancer protective
• Improved insulin sensitivity
• Increased PGC1 alpha
• Decreased inflammation
• Reduces oxidative stress
• Rids body of excess fluid
• Improves adaptive responses
• 3 week alternate - day fasting
• Improved fat oxidation
• Improved weight loss
• Improved insulin sensitivity
• Improved HDL
• Triglycerides decreased
• Improved adiponectin (37%)
• Glycine
Neurotransmitter Regulation:
• Glycine acts as an inhibitory neurotransmitter in the central nervous system,
playing a role in modulating neuronal activity and promoting relaxation.
• It can counteract the effects of stimulating neurotransmitters, such as glutamate,
and help regulate the balance between excitatory and inhibitory
neurotransmission
Melatonin Depleted by
• Beta-blockers
• Calcium channel blockers
• Benzodiazepines
• Estrogen-containing medications
• Hydralazine
• Loop diuretics
• Theophylline
• Antidepressants, including SSRI (Selective serotonin reuptake inhibitors)
• NSAIDs (Non-steroidal anti-inflammatory drugs)
Extracellular Matrix
• The extracellular matrix is a supportive network comprised of
connective tissue, collagen fibers, water, lymphatic vessels, and all the
tributaries in the lymphatic system that creates the environment
between and around cells.
• It is not just for the physical support of the cells, but also is integral to
the function and behavior of the cells in many different ways.
• It controls the life cycle of the cells.
• Modulates and influences how growth factors are utilized; 15 - 20
growth factors are regulated in the ECM such as glycoproteins.
• The ECM is a three-dimensional network that contains all the organs,
tissues, and cells of the body, playing a fundamental role in
protection, nutrition and cell innervation; it is the substrate where
the response of the immune system takes place, angiogenesis,
fibrosis, and tissue regeneration occur.
• Receives Innervation from the free endings of the ANS fibers, which
behave as a synapse with the cells of the matrix and parenchyma.
• The alteration of the ECM will lead to a loss of its function, affecting a
correct immune response to infectious, tumor and toxic agents.
Definition of Neural therapy
• Injections of local anesthetic in low concentrations in specific points
of the nervous system with therapeutic and diagnostic purposes
• Specific points based on the patient’s clinical history
• The main objective is to eliminate irritations of the nervous system,
primarily of the autonomic nervous system to restore its regulatory
function
Procaine
Neural Therapy technique primarily involves the injection of local anesthetic
called Procaine (Novocain) into scars, trigger points, tendon and ligament
insertions, peripheral nerves, autonomic ganglia, and different tissues
It is hydrolytically broken down within a few minutes by plasma
cholinesterase.
It is used in the form of Procaine Hydrochloride diluted to 0.5% or 1%, without
excipients and without mixing
Vasodilation , anti inflammatory, anti rheumatic, improves coronary
perfusion, negative inotrope, antiarrhythmic, antimicrobial anti cancer
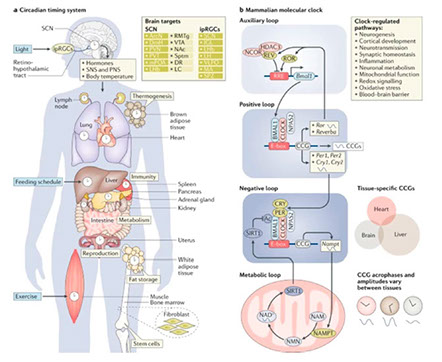
Andarine (S4, GTX-007)
• Developed for muscle wasting
• Reported to help maintains cortical bone content
• Improve Bone mineral density
• May reduce risk of fracture
• Weight loss
• BPH (benign prostatic hypertrophy) - reduces prostate
size/weight
• Is often “stacked“ by users
• Andarine competitively blocks DHT to prostate receptor
targets
• Partial androgen receptor agonist – helps decrease SEs
associated with anti-androgens researched for BPH
• Primary SE’s of andarine are:
• Disturbed vision – yellow-tinged color
• Suppression of testosterone
Growth hormone
Growth hormone (GH) is secreted by the anterior pituitary
a major stimulant in somatic growth control
a pleiotropic hormone that affects bone and muscle mass, carbohydrate, fat, and
protein metabolism, sexual maturation, and insulin resistance
Involved in immune regulation, and the GH receptor is expressed by several leukocyte subpopulations, mediates thymic development, promotes T cell engraftment in severe combined immunodeficiency mice, improves B cell responses and antibody production, and modulates NK cell and macrophage activity as well as in vivo Th1/Th2 and humoral immune responses
Reduces Type I DM development by altering tolerization mechanisms such as the cytokine environment, macrophage polarization, activation of the suppressor T cell
population, and Th17 cell plasticity
Gonadorelin
• Gonadorelin is a decapeptide
• A Key Regulator of Reproductive Hormone Signaling
• It acts as a key regulator in the hypothalamic-pituitary-gonadal (HPG) axis, which is
responsible for the control and release of reproductive hormones.
• It shares structural similarities with GnRH, which is produced in the hypothalamus
of the brain.
• The hypothalamus releases gonadorelin into the hypothalamic-pituitary portal
system, where it travels to the anterior pituitary gland.
Mechanism of Action:
• Gonadorelin binds to GnRH receptors on the surface of gonadotroph cells in the
anterior pituitary gland.
• This binding triggers a signaling cascade that results in the release of folliclestimulating hormone (FSH) and luteinizing hormone (LH) from the anterior
pituitary.
Regulation of Reproductive Hormones:
• FSH and LH, released in response to gonadorelin, act on the gonads (ovaries in
females and testes in males) to regulate gametogenesis (the production of
gametes) and steroid hormone production.
• In females, FSH stimulates the development of ovarian follicles and the production
of estrogen, while LH triggers ovulation and promotes the formation of the corpus
luteum.
• In males, FSH stimulates spermatogenesis (the production of sperm), while LH
stimulates the production of testosterone by the Leydig cells in the testes
Clinical Applications:
• Gonadorelin has various clinical applications in diagnosing and treating disorders
of the HPG ( hypothalamic- pituitary gonadal )axis.
• Gonadorelin stimulation tests are used to assess the functionality of the HPG axis,
providing valuable information in cases of delayed or precocious puberty,
infertility, and hypothalamic or pituitary disorders.
• Therapeutically, gonadorelin can be administered to restore or enhance
reproductive hormone levels in individuals with hormonal deficiencies or to induce
ovulation in assisted reproductive technologies
• Prevent testicular shrinkage
• Treats lack of testicular development
• Increases libido
• Improves mood
• Regulate testosterone levels
• Muscle health
• Helps testosterone levels stay optimized when taking prescribed testosterone
therapy.
• Dosage
• Gonadorelin 5ml vial 2mg/ml injection ( 100mcg) two to three times per week ,
dosage vary among patients depending on the case
potential side effects
• Allergic reaction such as skin rash, nausea, hives
• Stomach pain
• Dizziness
• Swelling of the lips
• Some female patients have referred water retention and headaches with the use
of gonadorelin
Ghrelin
28-amino-acid naturally-occurring peptide
Anti-inflammatory prosperities of ghrelin are due to it modulating the secretion of proand anti-inflammatory cytokines from LPS-stimulated macrophages
Exogenous ghrelin significantly augmented the release of the anti-inflammatory cytokine IL-10
Waseem, T. “Exogenous Ghrelin Modulates Release of Pro-Inflammatory and Anti-Inflammatory Cytokines in LPS-Stimulated Macrophages through
Distinct Signaling Pathways.” Surgery 143, no. 3 (March 2008): 334–42.
Ghrelin decreased both the clinical and histopathological severity of the colitis
and increased the survival rate. These effects seem to be attributable to the
decrease of both inflammatory and Th1-driven autoimmune
responses via affecting several inflammatory mediators, and by the
involvement of IL-10/transforming growth factor-ß1-secreting regulatory T cells
Lingandrol (LGD-4033)
• Anabolic support
• Supports skeletal muscle mass/strength
• 0.1-1.0 mg orally QD x 3-6 wks when supporting
metabolism
• Can increase to 5-10mg orally QD x 12 weeks for
performance enhancement
• There may be risk of testosterone suppression at doses
greater than 10 mg
• Many online blogs tout Ligandrol as being extremely
effective for:
• Enhancing performance
• Bulking (vs. cutting)
• muscle hardening
• Increasing vascularity
• Gaining size
• Enhancing recovery
Nicotinamide Adenine Dinucleotide (NAD+)
- crucial amino acid and
coenzyme of Niacin (Vitamin B3) that is found in every cell of your body.
• One of the most impacted organs from NAD+ deficiency is the brain.
• Brain renovation
• Replenishes neurotransmitters
• Improve cognitive functioning
• overcome anxiety, depression, chronic or acute stress, and other conditions
by giving the brain what it needs to return to proper functioning.
• It has a powerful capacity to reset the brain to its original set point.
• NAD+ is a coenzyme for redox reactions, making it central to energy
metabolism.
• NAD+ is also an essential cofactor for non-redox NAD+-dependent
enzymes, including sirtuins, CD38 and poly(ADP-ribose) polymerases.
• NAD+ can directly and indirectly influence many key cellular
functions, including metabolic pathways, DNA repair, chromatin
remodeling, cellular senescence, cognition and immune cell function.
These cellular processes and functions are critical for maintaining
tissue and metabolic homeostasis for a healthy ageing
Sirtuins and NAD+
• Sirtuins are a family of signaling
proteins involved in metabolic
regulation.
• These proteins utilize NAD+ to
maintain cellular health and
turn NAD+ to nicotinamide
sirtuins are implicated in
influencing cellular
processes like aging,
transcription, apoptosis,
inflammation, and stress
resistance, as well as
energy efficiency and
alertness during lowcalorie
situations
sirtuins are critical for fine-tuning of hormone sensitivity. These
sirtuins, when activated, play a critical role in modulating the
responsiveness of hormone receptors.
• sirtuins can enhance the sensitivity of estrogen receptors (8).
• When sirtuins are activated, estrogen receptors are more receptive to
the estrogen being produced by the body, meaning that estrogen can
be utilized to perform its critical functions. This heightened sensitivity
can be particularly important for regulating the menstrual cycle,
maintaining bone density, and influencing mood.
• sirtuins also play a role in influencing androgen receptor sensitivity
(9). By supporting androgen receptor responsiveness, sirtuins can
impact the body's ability to respond to testosterone. This affects
muscle mass, bone density, and overall vitality in men.
• NAD+ acts as the essential activator of sirtuins. Since sirtuins cannot
carry out their roles effectively without an adequate supply of NAD+
it is critical to maintain healthy NAD+ levels to support sirtuindependant
hormone functions during aging.
NAD+ and Testosterone
• NAD+ plays a critical role in testosterone synthesis by actively
supporting the activity of a key enzyme called 3β-Hydroxysteroid
Dehydrogenase (11). This enzyme is required for the biosynthesis of
all classes of steroid hormones, including testosterone (12). In
essence, 3β-Hydroxysteroid Dehydrogenase is a key player in the
transformation of precursor molecules into testosterone.
• With sufficient NAD+ levels, this enzyme can efficiently carry out its
role, ensuring that precursor molecules are effectively converted into
testosterone
NAD+ and Estrogen
• NAD+ is related to estrogen levels through its intricate relationship
with the enzyme 17β-Hydroxysteroid Dehydrogenase. This enzyme is
important for the metabolism of estrogen, playing a pivotal role in the
conversion of estrone to estradiol, the biologically active form of
estrogen. Importantly, NAD+ serves as a coenzyme for 17β-
Hydroxysteroid Dehydrogenase, actively participating in the chemical
reactions that enable this conversion
NAD+ and the Thyroid
• NAD+ is crucial for maintaining the balance of T3 and T4 levels in the
body due to NAD+ being required for sirtuin activation. Adequate
NAD+ levels also support the proper functioning of thyroid enzymes,
ensuring the synthesis and conversion of thyroid hormones occur
efficiently.
• the conversion of T4 to T3, a critical step in thyroid hormone function,
is facilitated by enzymes like type 2 deiodinase (D2), which are NAD+-
dependent.
Ostarine (MK-2866)
• AKA Enobosarm (GTX-024)
• Anabolic support
• Cancer cachexia
• Increases lean body mass and muscle performance
• Enhanced performance
• Improved fat loss
• Increased bone mineral density
Oxytocin Peptide
• 9 amino acid neuropeptide hormone
• 6 min half life
• FDA approved
• Declines with aging
• Epigenetic effect
• Positive effect on Mio carding contraction
(keeps contractibility of the heart).
• Anabolic effect on bone and muscle and
catabolic effect on fat.
Oxytocin Anabolic Peptide
• Love hormone
• Stimulated in labor, contact mother baby.
• It has been used to stimulate sex drive and libido in women.
• It has shown that stops and reverses osteoporosis and osteopenia.
• Glucose regulatory effects.
• It has protective effect on the brain.
• Oxytocin never triggers cancer.
• SAFE
• Stimulation of Osteoblast Activity: Osteoblasts are cells responsible
for bone formation. Studies have shown that oxytocin receptors are
present on osteoblasts, indicating that oxytocin may directly stimulate
bone formation by increasing osteoblast activity. This could lead to
increased bone density and strength, potentially reversing
osteopenia.
• Inhibition of Bone Resorption: Oxytocin may also play a role in
inhibiting bone resorption, the process by which bone tissue is broken
down and minerals are released into the bloodstream. By reducing
bone resorption, oxytocin could help maintain bone density and
prevent further bone loss associated with osteopenia.
• Regulation of Calcium Metabolism: Oxytocin has been shown to
influence calcium metabolism, which is essential for bone health. By
regulating calcium levels in the body, oxytocin may contribute to
maintaining optimal conditions for bone mineralization and
preventing calcium loss from bones.
• Stops and reverse osteoporosis and osteopenia.
PE -22-28 peptide
PE-22-28
• Is a synthetic derivative of the naturally occurring peptide spadin.
Spadin is a secreted peptide derived from sortilin.
• Antagonist of the TREK-1 ( TWIK- related-potassium channel) receptor
two-pore potassium channel identified as a potential target in the
treatment of depression and as a possible neurogenic regulator.
• PE-22-28 is the representative peptide for this group of synthetic
spadin analogs
• Has been shown to be more stable and have improved antidepressant
activity and neurogenic properties over the naturally occurring spadin
• PE-22-28 has been shown to induce neurogenesis after 4 days, which
is substantially faster than any known antidepressant.
• Useful in other applications such as learning, stroke recovery and
neurodegenerative diseases
TREK-1
• Is the receptor that spadin and PE-22-28 primarily bind to
• Is found in regions of the brain controlling mood, memory, and
learning, these areas include the prefrontal cortex, the amygdala, and
the hippocampus.
• Helps to protect against excitotoxicity
• Depression
PE-22-28 has been shown to relieve
depression in just 4 days without
producing any side effects on other
functions that are controlled by the
TREK-1 channel
TREK-1 receptor has been implicated
in pain sensitivity, seizure activity, and
cardiac ischemia. Research in mice,
however, shows none that none of
these side effects are observed in the
use of PE-22-28
Neurogenesis
• Research with PE-22-28 shows that this peptide can upregulate
neurogenesis, but in shorter duration of time, than regular
antidepressants
• studies show that PE-22-28 increases both neurogenesis and
synaptogenesis after just 4 days.
• In the case of synaptogenesis PE-22-28 appears to double the rate of
synapse formation
PT 141 Bremelanotide Acetate
• Also known as Bremelanotide, is a synthetic peptide that acts as a melanocortin
receptor agonist. It was initially developed as a potential treatment for sexual
dysfunction and has gained attention for its potential effects on sexual arousal and
desire.
• PT-141 works by stimulating the melanocortin receptors in the brain, specifically
the MC4 receptor, which is involved in the regulation of sexual function. By
activating these receptors, PT-141 increases the release of dopamine, a
neurotransmitter associated with pleasure and reward, in the brain. This
mechanism of action is thought to enhance sexual arousal and desire
• Melanocortin receptor agonist
• Analog of alpha MSH (melanocyte
stimulating hormone)
• Ac-Nle-cyclo[Asp-His-D-Phe-Arg-Trp-
Lys]-OH
• FDA approved for female hypoactive sexual desire disorder (trade name Vyleesi©,
Palatin Technologies, NJ)
• Also beneficial in male sexual dysfunction issues
• Erectogenic properties
• Unlike Viagra, PT-141 targets the neurological system vs. vascular
• PT 141 is agonist of MC-4R promoting feeling of satiety and decrease appetite
• It is estimated that 43% of women (30 million is the US) suffer from
sexual dysfunction and 30 million men suffer from ED, with incidence
increasing 2-3 x between ages 40-70
• PT-141 currently has no contraindications and is 80% effective in
people who don’t respond to Viagra or Cialis
• 2mg (0.2ml) starting dose, 45 minutes - 1 hour before sex
• Men should start at 0.1ml and titrate up to and not exceed 0.2ml.
• Recommended to inject 1mg (0.1ml) for test dose, then add 1mg (0.1ml) more 30
minutes later
• Women should start at 0.2ml dosing protocol.
• Duration of effects after administration is 24-72 hours
• Dose 2 x weekly initially, then may increase if tolerated
• Discourage the concurrent use of any PDE5 inhibitor with patients when using PT-
141
Dr
Testolone – RAD-140
• Primarily researched for muscle wasting and breast cancer
• Neuroprotective in lab studies
• Reported to inhibit the growth of androgen/estrogen receptorpositive
breast cancer models
• Additional SE’s from other SARMs is insomnia and lethargy
References