
Pancreas Cytology
General
Normal pancreas
General
If a mass is highly suspicious on imaging, should just be resected; otherwise cytology may be appropriate
- significant morbidity of surgery; not all lesions tx'd c surgery (ie lymphoma)
- FNA can be through skin or done endoscopically (more common bc allows for staging sometimes)
- up to 3% complication of acute pancreatitis
- cysts are traditionally hypocellular
- bile duct brushing best eval'd by liquid-based prep; smears can be air-dried or EtOH-fixed
- biochemical analysis can be done on cysts
Categories for reporting: Negative for malignant cells; Atypical cells present; Suspicious for malignancy; Neoplastic cells present; Positive for malignant cells; Nondiagnostic specimen
Normal pancreas
Normal pancreatic tissue has little stroma and lots of parenchyma
- exocrine tissue arranged in ducts around lobules that inc in size as approaches ampulla
-- mucinous differentiation indicative of PanIN
- acinar cells > ductal cells (opposite in bile ducts)
Cyto: acinar cells in grape-like clusters and isolated cells attached to fibrovascular stroma c eccentric round nuclei; evenly distributed finely granular chromatin c abundant cytoplasm and indistinct cell borders (+ SYN, CHR, CD56)
- ductal cells in evenly-spaced flat sheets (honeycomb, not usually single cells) c round nuclei; finely granular chromatin; no nucleoli and well-defined cytoplasmic borders (+ PAS-D, amylase)
- any cytoplasmic mucin is pathologic
Acute Pancreatitis
Caused by release of enzymes that hurt the pancreas, is rarely aspirated
- if aspirated, may see neutros, calcifications, necrotic debris and histiocytes

Normal pancreatic acinar cells c eccentrically located round nuclei and abundant cytoplasm

Normal ductal cells, in sheet arrangement, showing round nuclei and relatively little cytoplasm (from pathologyoutlines.com)
Chronic Pancreatitis
May mimick a neoplastic process bc forms a fibrous mass; thus if aspirated will be hypocellular c inflam and fat necrosis / calcifications, flat sheets of evenly-spaced cells that are mildly crowded, no (or rare) atypical cells, round nuclei c smooth nuclear contours, prominent (but not macro-) nucleoli, rare mits and low NC
IHC: (+) SMAD4 (lost in carcinoma)
- negative p53 (accumulates in carcinoma)

Pseudocyst
Usually caused by acute pancreatitis; lacks an epithelial lining (hence "pseudo-") but has an inflammatory fibrous capsule which surrounds necrotic tissue
- cyst fluid has inc amylase, CEA is low
pancreatic pseudocyst
Serous Cystadenoma
Up to 2% of pancreatic tumors, is subclassified based on number and size of cysts; serous microcystic adenoma being the most popular of these and occuring in women in 7th decade
Cyto: hypocellular, clean / bloody background, flat sheets and loose clusters of cuboidal cells c finely vacuolated / granular cytoplasm c indistinct borders, bare nuclei, small nucleus, fine chromatin and no nucleolus
Lymphoepithelial Cyst
Rare b9 squamous-lined cyst found in middle-aged men; assoc c HIV
Cyto: anucleate squamous c lots of keratinous debris; mature superficial squames, lymphs, cholesterol clefts
Mucinous Cystic Neoplasm (MCN)
5% of pancreatic neoplasms; found in the body / tail of pancreas women in 6th decade
- uni- or (usually) multilocular cysts, no communication with pancreatic ducts
- lining epithelium has a spectrum ranging from benign, borderline and malignant
Lined by mucinous epitelium that is completely enclosed and has ovarian-type stroma that expresses ER/PR
- may be considered malignant if there is some degree of invasion
- the ovarian-type stroma is rarely seen in cytology
IHC: (+) pVHL, S100P, DPC4, MUC5AC, MUC6+/-
Tx: excision (irrespective of grade)
Px: 1/3 assoc c invasive adenoca
MCN

Intraductal Papillary Mucinous Neoplasm (IPMN)
Rare, more freq in older males, MC in head of pancreas
- radiological and clinical input is essential
- single or multiloculated ducts
Up to 5% of pancreatic tumors
- grow along pancreatic ducts making thick mucin that can block pancreatic secretions and form cysts; usually found in head of pancreas; M=F
- similar to MCN, may be invasion (MCN and IPMN cannot be distinguished by cytology)
Px: excellent if no invasion; otherwise grade based on depth of invasion
Pancreatic Intraepithelial Neoplasia (PanIN)
Pre-malignant mucinous changes in the pancreatic ducts
PanIN-1 = low grade atypia
PanIN-2 = moderate atypia c stratification and tufting of epithelium; polarity is maintained
PanIN-3 = severe atypia w/o invasion (confined to ducts)
IHC: synapto,

Pancreatic Ductal Adenocarcinoma
MCC pancreatic neoplasia (up to 9/10); smoking is a risk factor; seen in 7th-9th decades presenting c abd pain, jaundice, pruritis, unexplained weight loss
- most (3/4) found in pancreatic head and most are well- to moderately diff
Cyto: hypercellular c irreg clusters (drunken honeycomb) and single cells c strange morphology (irreg contours and chromatin distribution), inc NC, mucinous cytoplasm, marked anisonucleosis (4:1 nuclear size variation in a single sheet / group)
- the groovy nuclei are sometimes called popcorn cells; and the grooves in cells sometimes called tulip cells
- some cells c foamy cytoplasm can have deceptively low NC
IHC: (+) p53, PanCK, E-cadherin
- negative (nuclear) SMAD4, synapto, chromogranin, vimentin, trypsin, lipase, NSE, PR, B-catenin, a1-antitrypsin, a1-antichromotrypsin, CD10, CD56, Chymotrypsin

Well-differentiated ductal Ac
Pancreatic Neuroendocrine Tumor (PanNET or PEN)
Up to 2% of pancreatic tumors; generally small circumscribed lesions seen around 5th decade
- can be low or high grade (well- or poorly differentiated, respectively); though cytologic atypia doesn't correlate c malignant behavior
May be functional and secrete variety of hormones (insulin, glucagon, VIP, serotonin, etc)
-- insulinomas are generally b9; though up to 4/5 are considered aggressive
- rarely invade pancreatic ducts
Cyto: hypercellualr c single cells (bare nuclei) in pseudorosettes or small clusters c uniform, round, eccentric (plasmacytoid) nuclei and salt n peppa chromatin
Proliferation rate used to grade:
Low-grade = 2-10 mits / 10 hpf
Intermediate-grade = 10-20 mits / 10 hpf
High-grade = >20 mits / 10 hpf
- Ki67 may be helpful
IHC: (+) Pankeratin, chromogranin, synaptophysin, CD56, Islet 1, PAX8;E-cadherin, may also stain for pancreatic hormones, variable vimentin
- negative trypsin, B-catenin (can see membranous or cytoplasmic staining), lipase, a1-antitrypsin, a1-antichymotrypsin, CD10
Px: cytologic atypia does not correlate with malignant behavior, with the exception of high-grade small and large cell neuroendocrine tumors
- most reliable predictor is presence of invasion or mets
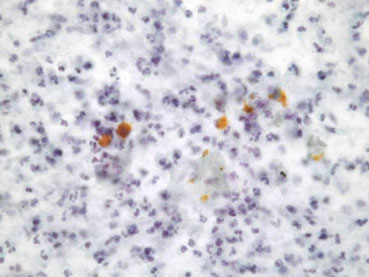
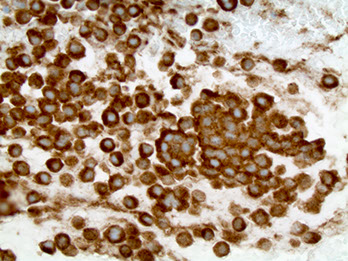
Pancreatic neuroendocrine tumor
PanNET (SYN+)

Neuroendocrine Tumor

Acinar cell Carcinoma (ACC)
<2% pancreatic neoplasms; occurs around 7th decade; can be anywhere in pancreas
Resemble pancreatic acini and make pancreatic enzymes; usually solid
- can be functional, secreting lipase, amylase,
Cyto: hypercellular c solid-cellular pattern of monomorphic single / naked cells in non-cohesive aggregates c granules in background, round / oval nucleus c smooth contour, prominent nucleolus and delicate granular cytoplasm
IHC: (+) Pankeratin, trypsin; lipase, a1-antitrypsin, a1-antichymotrypsin, weak B-catenin; usually positive for Islet 1 and PAX8, B-catenin can be membranous
- negative chromogranin, synaptophysin, CD56, vimentin
Px: poor; <10% 5-year survival

Acinar cell carcinoma (ACC)
Solid-Pseudopapillary Neoplasm (SPN)
- aka Solid PesudoPapillary Tumor (SPPT)
Rare (up to 2%) in young women (around 4th decade) found throughout pancreas
Well-circumscribed c variable solid and cystic parts
Cyto: hypercellular c myxoid fibrovascular cores lined by tumor cells c finely vacuolated cytoplasm c indistinct cell borders and round nuclei c grooves and no nucleoli; hyaline globules that are PAS-D positive
IHC: (+) CD56, B-catenin (nuclear), KIT (CD117), CD10, vimentin, NSE, PR, a1-antitrypsin, a1-antichymotrypsin, chymotrypsin, variable Pan CK and synaptophysin
- negative E-cadherin, trypsin, lipase
Tx: surgery (usually curative)
Px: usually low malig potential, but may have invasion into structures (nerve, vessels) that suggest aggressive behavior
SPN

Pancreatoblastoma
Rare; found in young children (MCC pancreatic neoplasm in childhood)
Cyto: Epithelial part c syncytial groups and isolated cells that are monomorphic c moderate cytoplasm and squamoid corpuscles; also a stromal part c primitive spindly cells and occasional heterologous elements (ie cartilage)
IHC: (+) Pankeratin, trypsin, chromogranin, synaptophysin, CD56; weak B-catenin

Pancreatoblastoma metastatic to liver c squamous morula
References
1. Cibas