GI Tract Cytology
Esophagus
Stomach
Small Intestines
Colon
Esophagus
~25 cm tube stretching from pharynx to cardia of stomach
- pierces diaphragm and is posterior to trachea
- carcinoma of esophagus can invade aorta or trachea
- normally a non-keratinized stratified squamous c islands of gastric mucosa (columnar cells) in area of gastric cardia at entrance to stomach
- food particles (vegetable cells) can be seen if obstruction present
Specimen can be collected by blind lavage (washings) or endoscopy brushing (bx may rupture bc thin epithelium)
Micro: normally see
Chronic Esophagitis
- caused by corrosive agents, hiatal hernia, infx (tb, fungal, parasitic)
- sheds lots of small distorted parabasal squames, which single, clustered or in sheets c cytoplasmic nuclear molding, scanty basophilic cytoplasm, large centrally located nuclei, nuclei moderately irreg in shape, chromatin coarsely clumped and isolated, chromatin c tendency c tendency to migrate to the periphery, prominent nucleoli
- has sheets of highly reactive hyperchromatic parabasal cells c big nuclei, prominent but regular nucleoli, and uniformity in size and shape
- small parabasal cells seen in chronic erosive esophagitis
Herpetic Esophagitis
- relatively common viral inflam of esophagus
- assoc c administration of cortisone therapy, debilitated patients, contamination from buccal cavity or resp tract
Acute gastritis
Main cellular component is inflam cells; only a few single epithelial cells present; gastric cells occasionally seen c round pale nuclei, enlarged nuclei, prominent nucleoli, and uniformity in size and shape
Peptic ulcer
Large number of epithelial cells c bare nuclei that are uniform in size and round or oval in shape
- goblet cells are present, as well as gastric cells c some atypia that have moderate nuclear hypertrophy, coarse chromatin clumping, one or more small round nucleoli, overall cell regular size and shape and smooth nuclear membrane
Intestinal metaplasia
Normal gastric cells can be replaced by goblet columnar cells
- often present c straight line resembling terminal bar, cytoplasm often over-distended c secretory vacuoles (resembling signet-ring cells), nuclei uniform in size and shape, definite nuclear membrane, nucleoli are not prominent
Squamous cell carcinoma
Has well-differentiated nuclei, abundant orangeophilic cytoplasm, irregular pyknotic nuclei
Poorly differentiated carcinoma
Single cells to large sheets c scanty basophilic cytoplasm, large hyperchromatic irregular nuclei, abnormal chromatin clumping, wrinkled nuclear membrane
Stomach
Made of simple tubular glands
- mucus-making cells line the surface and neck of the glands in fundus and body of stomach
- deep portions of the glands have pepsin-producing chief cells and HCl-producing parietal cells
- pyloric area glands are uniformly lined by mucus-producing cells
- chief cells and parietal cells are not distinguishable from other columnar cells in routine cytologic specimens
- gastric brushing specimens have cohesive fragments of epithelium
- nuclei are small and uniform
- gastric lavage specimens (washings) have scant cell population in the absence of disease
- clusters of mucus-producing cells c honey-comb appearance is MC presentation of b9 gastric cells
- relatively uncommon single gastric cells have abundant cytoplasm c a flattened surface c opposite end tapering in a tail shape
-- nucleus is round c somewhat opaque centrally located and sometimes nucleolus present
- bare nuclei can be seen if cytoplasm destroyed or separated
- cells from resp tract or upper alimentary tract often present as well as plant cells
- leukocytes and lymphocytes in varying numbers can be present
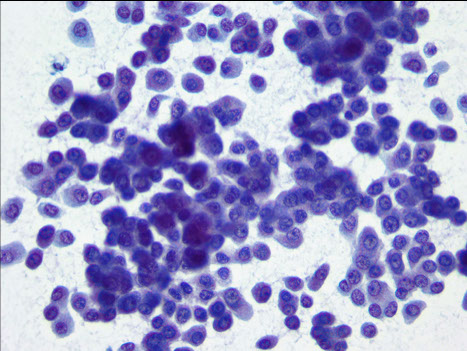
Well-differentiated Adenocarcinoma
Cells shed in tight clusters of large sheets; cell size and shape is variable and irregular, with marked intracellular molding, and cells usually larger than normal with variable size
- has abundant cytoplasm, often vacuolated; the mucin-containing vacuoles often mold the nucleus into a crescent shape (signet-ring cells); has delicate cytoplasmic membrane, well-defined and irregular
- single or multiple nuclei that are hyperchromatic, sharp, eccentric and have irreg borders
- coarse, clumped chromatin c large prominent nucleoli
Poorly-differentiated adenocarcinoma
17/20 shed numerous cells, 1/10 in loose clusters, 1/20 in sheets
- oval to round shape c scanty, poorly preserved cells, transparent or basophilic cytoplasm c ill-defined borders
- irregular shape c large nuclei, nuclear membrane c freq indentation or lobulations; has coarse chromatin that is usually unevenly distributed
- prominent nucleoli (60% of cells)
Linitis plastica
Very scanty numbers of epithelial cells which are always single
- cytoplasm is very scanty and transparent, cells are irregularly shaped c poorly-defined cellular borders
Gastrointestinal Stromal Tumor
Recapitulate differentiation toward interstitial cells of Cajal, the c-kit expressing pacemaker cells of the GI tract
Micro: oval nuclei c bland chromatin and inconspicuous nucleoli
IHC: (+) c-kit (CD117) and DOG-1
- DOG-1 is more sensitive than c-kit
Genes: most arise from mutations in c-kit gene, that encodes a transmembrane receptor for a stem cell growth factor
Tx: metastatic and inoperable GISTS show response to c-kit TKI imatinib (Gleevec)
Lymphoma
Sheds lots of diagnostic cells c very scanty cytoplasm, prominent nucleoli, coarsely clumped chromatin, irregular thick distinct nuclear membrane
- may be difficult to dx bc: can look like reactive lymphs seen in chronic inflam conditions (gastritis), or may look a lot like small cell poorly-diff adenoca, however adeno can have more cytoplasm
- Ddx: Pernicious anemia: enlarged cytoplasm and nuclei of gastric cells similar to those in cancer, but have bland appearance and very little contrast bwt staining of nucleus and cytoplasm
-- peptic ulcer: reactive nuclear features and general arrangement of cells =sugest a tissue-sheet, whereas in contrast carcinoma cells adhere less well and "tent", cells also tend to be fairly uniform in size and shape (not as pleomorphic as in carcinoma)
GIST

Small Intestines
B9 duodenum
- cell yield scant in absence of dz; few leukocytes or macrophages
- duodenal lining cells can not be differentiated from pancreatic or bile duct cells
- cells can be single or in clusters, have columnar shape c flat, sometimes ciliated surface, they are large, have round, clear and basally located nuclei and usually a small nucleolus
- arranged as "honeycombs" when in flat clusters, have opaque, sometimes finely vacuolated cytoplasm, either acidophilic or basophilic and occasional goblet cells
Inflammation in duodenal aspirates
Specimens usually more cellular and preservation is poor
- "A" pattern smear have small round degenerating epithelial cells and sometimes lots of leukocytes
- "B" pattern smears have a large number of naked nuclei and is assoc c chronic pancreatitis; goblet cells inc in chronic duodenitis
- Giardia lamblia can be seen in duodenal aspirates
Carcinoma in duodenal aspirates
MC tumors in this area are pancreatic (can do surgery if only the head of the pancreas involved; most other stuff is fatal)
- the source of cancers found in duodenal-pancreatic aspirates usually not distinguishable bc they all look similar
- usually see lots of necrotic debris and WBCs
- can have large hyperchromatic nuclei c cells single or in clusters, c papillary groups sometimes seen; usually c large, multiple irregularly-shaped nucleoli and have abundant cytoplasm in well-diff adenoca
Colon
Normal
colorectal cytology useful for high-risk pts (c familial polyposis of colon, UC and colon ca s/p tx) and to clarify unclear x-ray / colonoscopy findings
- the colonic mucosa made of single to double layer of columnar cells in tubular glands
- goblet cells numerous, c intervening cells c opaque cytoplasm
- cytology specimens can be made of scanty columnar cells , goblet cells, macrophages, leukocytes, squamous cells of anal origin and some dibris
Inflammation of the colon
Cytologic dx of cancer may not be possible 2/2 excessive inflam and debris, which can be difficult esp in pts c UC (who have inc risk of ca)
Reactive columnar cells usually bigger than normal, are pleomorphic and have large sometimes irregular nucleoli
- flat premalignant lesions can occur in UC, and cells brushed from these can look malignant; b9 polyps usually can not be id'd as such c certainty in cytology preps
Colon carcinoma
Adenomatous polyps and villous papilloma (another polypoid lesion) considered premalignant
- colon ca's are mucus-producing adenocas varying from well-diff to poorly-diff anaplstic tumors
- signet ring ca is a type of well-diff colon ca
Micro: large hyperchromatic nuclei, prominent nucleoli, poorly preserved cytoplasm that is variable in amt
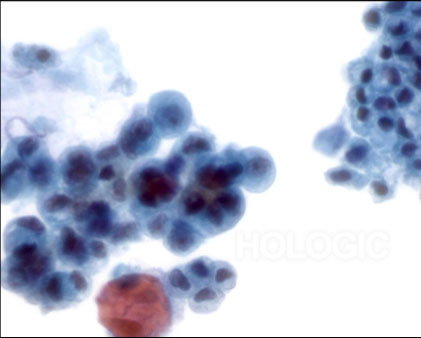
Hepatocellular Ca
- Aspirate of hepatocellular carcinoma in which hepatocytes and peripherally located endothelial cells are noted.
- Endothelial cells are characterized by spindle shaped cells having elongated nuclei and indistinct cytoplasm


Primary Sclerosing Cholangitis
PSC - false positive findings
Reactive ductal epithelium is associated with pancreatitis and cholangitis, it is important to distinguish from ductal adenoca
A high threshold for malignancy is needed for patients with:
-Primary sclerosing cholangitis
-Primary biliary cirrhosis
-Stones
-Indwelling stent
Mitoses, prominent nucleoli and nuclear enlargement are common to both reactive and malignant epithelium
Variation in nuclear diameter more than 3 or 4 fold within a group favors a malignant diagnosis

Benign, reactive ductal cell atypia
Pancreatic adenoca
Irregularly sized and shaped clusters and isolated cells
Uneven distribution of ductal cells within a sheet (“drunken honeycomb”)
Irregular nuclear contours and irregular chromatin
Anisonucleosis (>4:1 variation in diameter in a single sheet)

Pancreatic Neuroendocrine Tumor
The aspirates show single and dyshesive clusters of neoplastic cells
Cells show mild variation in size and have eccentrically located oval nuclei (plasmacytoid appearance). “Salt and pepper” chromatin
Few small cytoplasmic vacuoles are seen.