
Ear
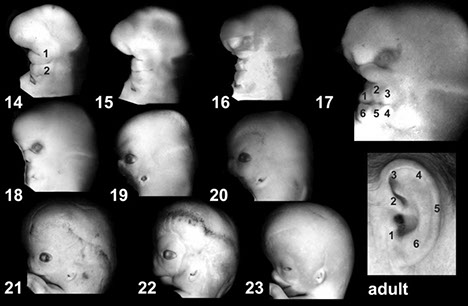
Embryology
Anatomy
Histology
Chronic Otitis Media with Glandular Inclusions
Angiolymphoid hyperplasia with eosinophilia
Cholesteatoma
Ceruminous Adenoma
Middle Ear Adenoma
Embryology
asdf
Anatomy
asdf
Histology
asdf
Chronic otitis media with glandular inclusions
Reactive non-neoplastic proliferation of the middle ear epithelium assoc c recurrent bouts of otitis media
- Presents with decreased auditory acuity. A nodular
proliferation of soft tissue is seen in the middle ear space
- may be mistaken clinically or histologically for a
neoplasm
Micro: Fibrous stroma with chronic inflammatory cells
and plump fibroblasts with microscopic cystic glandular spaces lined by flatted cuboidal epithelium (pinched off buds of the middle ear mucosal lining)
- widely scattered and lack the orderly pattern of a
neoplasm.
DDx: Ceruminous adenoma, middle ear adenoma.
Angiolymphoid hyperplasia with eosinophilia
Nodular vascular proliferation and inflammatory process, usually in skin of periaural region. M = F,
- Most in 3rd decade.
- Sx: itchy papules with tendency to bleed when scratched. Papules may coalesce into plaques.
- Similar histology seen in Kimura’s disease, but clinical is different: seen in Asian males, with associated lymphadenopathy and peripheral eosinophilia
Micro: Proliferation of small vessels with plump
epithelioid endothelial cells, surrounded by dense
lymphohistiocytic infiltrate with eosinophils. Germinal
centers often give impression of lymph node, but they are in soft tissue.
Tx: local surgical excision. May resolve spontaneously
Cholesteatoma
Invasive pseudoneoplastic squamous proliferation in
the middle ear, M > F, Any age (some congenital), but most common in 3rd-4th decades
- can arise de novo or following otitis media
- Middle ear is usual site but rare cases arise in the external auditory canal.
Sx: Asymptomatic until extensive invasion of middle ear space and mastoid air cells; symptoms are hearing loss, ear discharge and pain.
Gross: resembles an epidermal inclusion cyst
Micro: stratified keratinizing squamous epithelium,
keratinous debris, fibrous connective tissue or granulation tissue
Tx: excision;
Px: Recurrence and progression may be extremely
destructive, even fatal.
- Complications: bone destruction, deafness, facial nerve paralysis, labyrinthitis, meningitis, brain abscess
- The bone destruction is caused by collagenase made by the squamous cells and by the connective tissue.
DDx: Cholesterol granuloma is different from cholesteatoma: it is the result of hemorrhage and contains cholesterol clefts and chronic inflammation
Ceruminous adenoma
B9 glandular neoplasm of the ceruminous (apocrine) glands of the external auditory canal
- Actually there are different ceruminous tumors:
1). Benign: ceruminous gland adenoma, mixed tumor,
syringocystadenoma, papilliferum.
2) Malignant: adenoid cystic carcinoma, ceruminous
gland adenocarcinoma, mucoepidermoid carcinoma
The ceruminous gland adenoma is seen more often in males and usually in the fifth and sixth decades
- present as a slowly growing mass in the external canal, with unilateral hearing loss.
Micro: two cell types line the well-formed glands
1) inner secretory layer with apocrine features
2) outer myoepithelial layer
- not encapsulated but well-demarcated
- Yellow-brown pigment may in the inner lining cells (cerumen)
Tx: excision
Middle ear adenoma
Rare; B9 glandular neoplasm arising from middle ear
mucosa; in any portion of middle ear
- Sx: unilateral hearing loss; also may have tinnitus, dizziness; rarely, pain and facial nerve paralysis
- Occasionally may perforate the tympanic
membrane and involve external auditory canal as well as middle ear
- M = F; most common in 3rd-5th decades
Imaging: avascular (distinct from paraganglioma)
Micro: unencapsulated, glandular proliferation with
various patterns
- Often reminiscent of carcinoid
- glands made of single layer of cuboidal to columnar cells with granular eosinophilic cytoplasm and round nuclei, often with salt and pepper chromatin. May have some pleomorphism, but mitoses uncommon.
- perineural invasion may be seen, even though benign.
IHC: (+) CK, EMA
- many (+) NE markers (CHR, SYN, S100, Leu 7)
Tx: : Complete excision
Px: can be locally aggressive, even lethal, no mets
Papillary neoplasm of endolymphatic sac origin
aka “Heffner tumor.”
Very rare, B9 but locally destructive tumor arising in temporal bone in area of endolymphatic sac
- originally described as a low-grade adenocarcinoma of endolymphatic origin, now “neoplasm”, since none have metastasized
- M = F, 2nd-8th decades; sx: unilateral hearing loss. Some cases are in patients with von Hippel-Lindau disease and this has become one of the lesions in the VHL complex
Micro: Papillary and cystic lesion with pink colloidlike
material in cystic areas. The papillae are lined by
cuboidal to columnar bland cells with pale eosinophilic to clear cytoplasm and uniform nuclei
- colloid-like material is PAS positive
IHC: (+) CK; negative thyroglobulin
DDx: Metastatic thyroid papillary carcinoma;
metastatic adenocarcinoma, especially renal cell
carcinoma, middle ear adenoma
Tx: Radical surgery, even with sacrifice of cranial nerves
- First chance is only chance and may be curative
Neurilemmoma of CN VIII
B9 nerve sheath tumor; accounts for over 90% of
cerebellopontine angle tumors
- F > M. 4th-7th decade most common. Association with neurofibromatosis. NF 2 patients develop these tumors earlier in life and are more likely to have bilateral tumors.
- usually arise just inside the internal auditory meatus, usually in the vestibular portion of the nerve.
Micro: Antoni A (compact spindle cell areas with nuclear pallisading in rows called “Verocay bodies.” Mitoses are few in number
- Antoni B: hypocellular myxoid areas
Ancient neurilemmomas may have bizarre nuclear atypia
IHC : (+) S100 strongly and diffusely positive
Tx: Complete surgical excision is curative.


References
1. Osler notes